Our study revealed that 9.9% (21/213) low-risk women with mid-trimester short cervix who delivered < 32 wks received only observation or were prescribed vaginal progesterone treatment, suggesting that building a predictive model is important for sPTB prediction and prevention. Furthermore, we incorporated maternal clinical characteristics, sonographic assessment of cervical length and maternal blood results to construct a noninvasive prediction model and a simple scoring system to predict the individual probability of sPTB < 32 wks for low-risk women with a short cervix in mid-trimester pregnancy. This innovative sPTB prediction model can potentially provide better predictive capacity and management strategies in clinical practice.
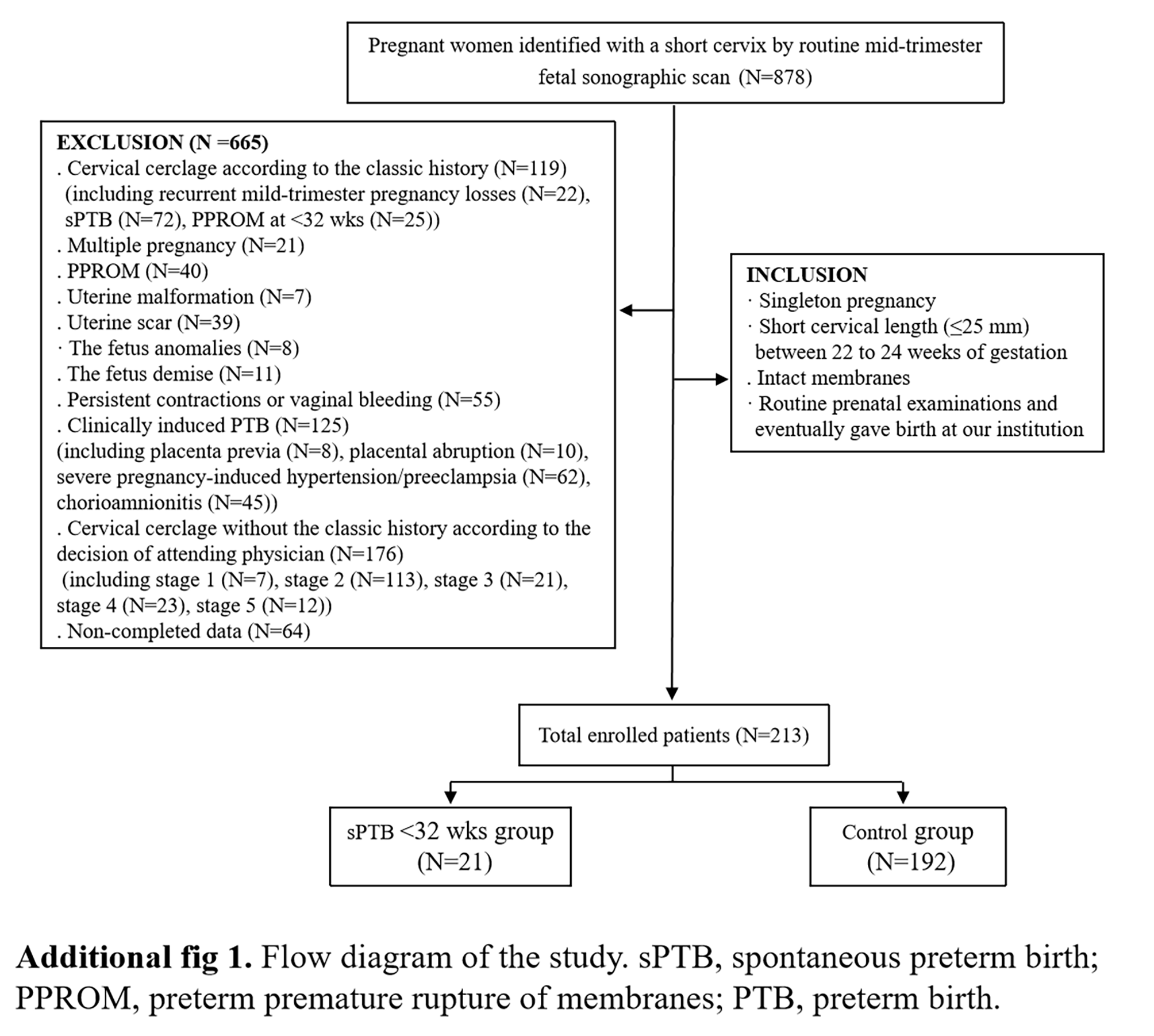
In women with singleton pregnancies without a history of sPTB, the incidence of CL ≤ 25 mm was 0.81-2%[16–18]. Our population was assessed using vaginal ultrasonography during the mid-trimester fetal ultrasound scan between 22 and 24 wks, which revealed that the prevalence of CL ≤ 25 mm was 1.6% and 0.4% in the low-risk population. Among the low-risk subjects, 42 delivered with sPTB, and 21 delivered before 32 wks. Hadar et al. reported that the total rate of sPTB before 32 weeks was 9.9% in asymptomatic singleton pregnant women11, but some women enrolled in the study underwent cervical cerclage, which might have led to bias in the actual incidence of sPTB.
A history of sPTB is a strong high-risk factor for sPTB. Accumulating evidence indicates that transvaginal sonographic CL measurement in mid-trimester pregnancy is also a key clinical tool for predicting the occurrence of sPTB. Therefore, the American College of Obstetricians and Gynecologists (ACOG) guideline recommend routine transvaginal CL screening from 16 to 24 weeks for women with singleton pregnancies and a history of sPTB. However, differences exist regarding further screening and management for singleton pregnant women with a short cervix without high-risk factors for sPTB[5, 9, 19–21]. Our data showed that 0.4% of the low-risk subjects had a CL ≤ 25 mm. These individuals underwent observation or received vaginal progesterone treatment, and 9.9% ultimately delivered prematurely < 32 wks; consequently, a predictive model for low-risk women with a short cervix will be constructed to allow for better management and interventions to prevent or delay sPTB.
Our study defined predictors, including multiparity, leukocytosis and a short CL, that are associated with the occurrence of sPTB < 32 wks. A short CL (< 15.5 mm) was the most significant independent predictor for sPTB. In a study of unselected pregnant women between 22 and 24 wks conducted by Heath et al., only 1.7% had a CL < 15 mm, but they accounted for approximately 58% of those with sPTB < 32 wks[22]. Additionally, multiparity, as a predictor, can underscore the complex relationship between parity and sPTB. Our study revealed that low-risk women who are multiparous are at high risk for sPTB < 32 wks. A retrospective cohort study by Koullali et al reported that the likelihood of sPTB occurring in nulliparous women was greater than that in multiparous women in their second pregnancy (OR, 2.15; 95% CI, 1.98–2.3)[23]. This conclusion contradicts what was observed in our study, which may explain the status of the population. Our study focused on low-risk women and might hypothesize that greater parity may increase the risk of sPTB < 32 wks due to a damaged cervix, which is consistent with the finding of Koullali that when analyzing multiparous patients with a parity > 4, the risk of sPTB < 32 wks increased with increasing parity (OR, 1.26; 95% CI, 1.13–1.41)[23]. Multiple studies have corroborated that elevated levels of inflammatory biomarkers are associated with an increased risk of sPTB. Various inflammatory biomarkers, such as matrix metalloproteinases, WBC, and CRP, have been studied in both the amniotic fluid and maternal serum for an association with the occurrence of sPTB[24–26]. Our study supports this reasoning, but the mechanism by which it impacts sPTB needs further exploration.
The bootstrap-corrected concordance index of our model was 0.815 (95% CI, 0.700-0.931), which indicates good predictive power and calibration. Cobo et al. included gestational age, CL, amniotic fluid glucose and interleukin (IL)-6 in a model for 358 women with a diagnosis of sPTB and intact membranes before 34 wks, and the ROC of the model for predicting the risk of sPTB within 7 days was 0.86 (95% CI, 0.77–0.95)[27]. Similarly, the ROC of the model developed by Watson et al. combined quantitative fetal fibronectin and CL in 689 asymptomatic high-risk women to predict sPTB < 34 wks was 0.76[28]. Compared with those of previous models, the main advantages of our model is that it focuses on low-risk pregnant women with a short cervix and excludes patients who undergo cervical cerclage, which could actually reflect the correct occurrence of sPTB. Additionally, our model is noninvasive and can be used clinically without the need for additional tests, which is cost-effective and acceptable.
In our study, risk group stratification using our score chart could clinically and noninvasively help clinicians more efficiently manage low-risk women with a short cervix in mid-trimester pregnancy. Table 3 shows the different clinical scenarios stratified by risk group. A total of 91.5% (195/213) of the patients were included in the low-risk group, and the actual rate of sPTB < 32 wks was 6.15%. Thus, the management of these patients could be reasonably limited to unnecessary interventions with a low-intensity intervention when necessary, such as observation. For the high-risk group, the actual rate of sPTB < 32 wks was 75%, and aggressive interventions could be a better choice to reduce the risk of sPTB and decrease the rate of perinatal deaths[29]. Nevertheless, evidence for the benefit of vaginal pessary use in select high-risk patients is limited. A randomized clinical trial conducted by Hoffman et al. in singleton pregnant women with a CL < 20 mm (n = 544) demonstrated that cervical pessary did not decrease the risk of sPTB and was associated with a higher rate of fetal mortality[19]. Thus, women in the high-risk group might require surgical interventions, such as cervical cerclage. Moreover, in the intermediate-risk group, the actual rate of sPTB < 32 wks was 42.86%. A meta-analysis indicated that in singleton pregnant women with a mid-trimester short cervix (n = 974), vaginal progesterone decreased the risk of sPTB < 32 wks[30]. The management of these intermediate-risk patients could be determined according to patients’ wishes, and the use of vaginal progesterone may be a better choice.
There is currently a lack of standardized management protocols for low-risk women with a short cervix in mid-trimester pregnancy with different individualized risk stratifications. In our study, we built a model for predicting the occurrence of sPTB in these women, further developed a classification system and provided optional management strategies. The validation of the nomogram and classification system remains essential for the scientific community. Additionally, studies exploring the efficacy of interventions in various risk groups based on the classification system are needed. These findings could help clinicians better identify, counsel and treat patients with various risk stratifications.
Our study has several limitations. First, the relatively small number of patients in sPTB < 32 wks group was a limitation of this retrospective cohort study, which may have confounded our data. Second, patients with visible dilation of membranes apparent in the internal cervical os were excluded from our study. This selection bias may have affected the performance of the model. Third, although we performed a rigorous internal validation, the model requires external validation using independent data sets to confirm its generalizability. Finally, one potential limitation in improving the predictive ability of a model is the lack of specific blood biomarkers. Future multicenter studies with larger sample sizes will be required before the model can be routinely used.
In conclusion, we constructed a noninvasive and efficient predictive model to predict the occurrence of sPTB < 32 wks in women with mid-trimester short cervix without additional risk factors for sPTB. The patients were divided into low-, intermediate-, and high-risk groups according to the score chart for risk stratification. Our nomogram and classification system may be useful for targeted interventions for women with a short cervix and without a history of sPTB, as unnecessary interventions should be reasonably limited to low-risk patients, and cervical cerclage might be considered for high-risk patients. Further prospective validation studies using independent populations will be conducted to evaluate the performance of the model.
{kind=link}