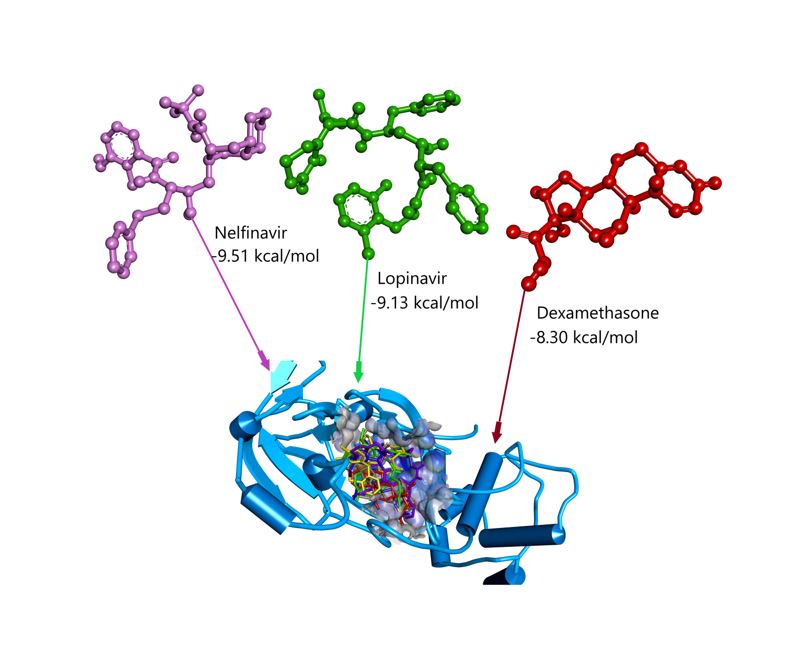
The previous studies have shown that nelfinavir may bind with other Mpro receptors such as 6LU7 and 3M3V. The BE results of these studies were -10.72 and -17.31 kcal/mol for 6LU7 and 3M3V. Although their tendency to interact poses was similar, the interactions of these complexes with each protein were different. In this study, nelfinavir interacts with the residues of amino acids GLN189, HIS164, PHE140, and GLU166, while it was bound with CYS145, MET49, MET165, GLU166, LEU167, PRO168, GLY170, GLN189, THR190, ALA191 and HIS41 in the active site of the 3M3V receptor 1. As a result, nelfinavir is often used as a standard for molecular docking research 6,7
Previous studies have shown that, lopinavir also has a functional inhibition of the Mpro receptor. In this research lopinavir is one of the top four, -9.13 kcal/mol. Although the BE score is higher than native ligand, this drug is reported as an inhibitor of the SARS-Cov-2 on Vero E6 cells with EC50 below 100 µM 21. This drug may be used in vitro against SARS-Cov, MERS-Cov, and hCov-229E 7. Lopinavir is often combined with ritonavir for inhibiting the Mpro receptor. This step causes the uses of lopinavir in a mixture that is not too much 7,22,23. The previous data showed that twenty-seven COVID-19 patients have treated with lopinavir 400 mg/ritonavir 100 mg 14. These drugs have also been reported to inhibit HIV protease, a member of β-coronavirus, due to their therapeutic benefits as antivirals. Lopinavir was shown to have the best therapeutic benefit compared to ritonavir 24. In addition to nelfinavir and lopinavir, the results of this study show that vitamin D in potent as an inhibitor of Mpro.
Vitamin D has the lowest BE among vitamins in this study, -9.12 kcal/mol. This vitamin is used in the treatment to improve the immune system of patients and as a preventive measures. Previous studies have reported that the use of vitamin D in therapy may reduce T helper cell type 1 (Th1) cytokines (tumor necrosis factor-α and interferon-γ) and expression of pro-inflammatory 25–27. The use of vitamin D in the Mpro receptor inhibitor reduces the expression of the dipeptidyl peptidase-4 receptor (DPP-4), a molecular virulent that reacts with the SARS-Cov-2 spike glycoprotein 28. However, there is no firm evidence of the relationship between vitamin D and the death of patients 12,13. Vitamin A has BE -7.99 kcal/mol and may also increase the immune system in the human body. This vitamin is included in the list of drugs used to treat and to maintain immune system stabilization in patients 29,30.
Vitamin E and C are also used as immune boosters for treatment with COVID-19 globally. The BE for vitamin E and C is -8.1 dan -4.08 kcal/mol, respectively. Both compounds are antioxidants that can be obtained from fruit and vegetables in our dietary menu. Also these antioxidants may be obtained from supplements. The BE of Vitamin E is lower than Vitamin C, so vitamin E is expected to be more strongly bound to the Mpro receptor. The previous study explained that this antioxidant might increase T-cell subsets, lymphocyte reactions to mitogen, interleukin-2 production, potentiated natural killer cell activity, and influenza virus response compared with placebo. The use of antioxidants in the therapy process is essential to maintain physical and spiritual conditions during the quarantine period, and the healing process is quickly completed 31,32.
The anti-inflammatory agent is included in the list of the drugs used for therapy because the immune response of COVID-19 patients has increased such as the number of leukocytes, platelets, lymphocytes, and neutrophils 33,34. Dexamethasone is one of the corticosteroid groups used to cure a patient of SARS-Cov infection in patients 19,35. Oxford University recently researched the use of dexamethasone to chronic patients in the United Kingdom (UK), and the WHO has accepted the results of the. Based on the previous research review, the corticosteroid group has been shown to have clinical benefit. Critically, genomic SARS-Cov-2 and SARS-Cov are similar, so a literature review is conducted to gather data and evidence on the efficacy of the drug in the treating of patients. The use of this drug is better than Non-steroidal Anti-Inflammation Drugs (NSAIDs) 35,36. In general, NSAIDs are used as a pain killer for acute to chronic inflammation. Long-term consumption of this drug may cause adverse cardiovascular events in the human body 16. Ibuprofen is one NSAIDs, and the use of these drugs causes an increase in ACE2 expression. The treatment of patients with co-morbid (diabetic) using NSAIDs may increase the incidence of SARS-Cov-2 infection 37. Researchers are still discussing COVID-19, followed co-morbid. The previous study reported that co-morbid (cancer) is not directly related to acute inflammation 38.
In addition to previous ligands, there are a number of other potential inhibitors such as umifenovir, darunavir, cobicistat, meropenem, midazolam, and levofloxacin. The BE of these ligands shall be between -7.83 and -7.0 kcal/mol. Generally, the BE of these potential inhibitors is higher than that of native ligand, but these inhibitors are still used for therapy. Umifenovir’s function is to inhibit the interaction of the virus with the host cell membrane 14. Umifenovir (arbidol) is used in vitro to cure influenza A infection. Applications of this drug to SAR-Cov-2 therapy still require advanced research to complete the information 39. Darunavir is also known as an inhibitor of HIV-1 protease, and this drug may prevent the dimerization of HIV-1 protease 40. In Atlanta, at dose of 800 mg darunavir/Cobicistat 150 mg, darunavir/cobicistat was used for 2 weeks (one daily) of patients 14. In addition to antioxidants, antibiotics are also used in the treatment of patients. Earlier work described that almost all patients received antibiotics, antiviral, and glucocorticoid. Meropenem and levofloxacin are mostly antibiotics used in the medication of COVID-19 victims 41–44.
Chloroquine phosphate, chloroquine, oseltamivir, chloroquine sulfate, hydroxychloroquine, cefotaxime, salbutamol sulfate, remdesivir, acetaminophen, ribavirin, favipiravir, vitamin C, and acetylcysteine have BE -6.55 to -3.51 kcal/mol. The BE of these potential inhibitors is higher than native ligand, so these drugs are expected to interact weakly with the active site of the Mpro receptor. Newly, chloroquine phosphate has an excellent clinical effect on the treatment of this viral virus, while the molecular docking calculation of this study is -6.55 kcal mol-1. Based on this score, this drug is weakly bound to the Mpro receptor 45.
Recently, a viral inhibitor has been used to treat patients with chloroquine, an antimalaria agent. The inhibition chloroquine mechanism on SARS-Cov-2 has not yet been invented. The previous study recommended that this drug be developed to treat COVID-19 with diabetes in India. The therapy was designed with a view to minimizing the risk, prolonged use, cost, and source of raw material 14. The coronavirus seems to be using hemaglutinin-esterase, which binds sialic acid to the surface of the glycoprotein. There is an indication that this virus interacts with ACE2. When this virus binds to ACE2, so this process will continue to replicate the virus. Chloroquine could well interfere with the mechanism of ACE2, and this drug inhibits the reaction with the target cell. Chloroquine may interfere with the biosynthesization of sialic acid. This drug also modulates the acidity of the endosome to prevent the formation of autophagosomes. When mitogen-activated protein (MAP) kinase activation is reduced, virus replication may be managed to stop. This potential inhibitor interfere in the maturation of protein M and the creation of virion before entering the host cell 9. The efficacy of this drug is to increase the pH of the endosome, a condition for the fusion virus 23.
Previous study reported that chloroquine demonstrated inhibition of Mpro receptor performance by indirect immunofluorescence assay. Inhibition of infection with this drug has been used to destabilize the terminal glycosylation of the cellular receptor, ACE2 46. Chloroquine is known to have been cheap and widely used 8,45. This drug may react with ritonavir/lopinavir in patient therapy 22,47. Eventually, chloroquine provides a good prediction for inhibition of Mpro receptor. This drug is generally used as an antimalarial drug 8. The previous study concluded that chloroquine was known as an antiviral agent for several viruses, including coronavirus OC43, enterovirus EV-A71, Zika virus, influenza A H5NI, SARS coronavirus, chikungunya virus (CHIKV), and Ebola virus. However, HIV therapy has not been recommended for this drug 8,23,48. In this study, chloroquine is not the best choice as a new potential inhibitor Mpro. It can not be considered a new potential inhibitor through the Mpro pathway because the BE of this ligand is bad.
Besides the potential inhibitor explained above, there are ligands that have to BE higher than native ligands such as oseltamivir, chloroquine sulfate, hydroxychloroquine, cefotaxime, salbutamol sulfate, remdesivir, acetaminophen, ribavirin, favipiravir, vitamin C, and acetylcysteine. Oseltamivir with the trademark Tamiflu was recognized as an antiviral agent that alters free carboxylate as an active metabolism 22,49. Apart from oseltamivir, many researchers suggest hydroxychloroquine as opposed to chloroquine because hydroxychloroquine has a low toxin level. In vitro, hydroxychloroquine was the most proposed drug than chloroquine 22,50. Since then, the USA has claimed that remdesivir can be used in the treatment of COVID-19 patients in their country. Subsequently, the recent study claimed that remdesivir had no clinical benefit from chronic COVID-19 51. This overview reveals that finding drugs or vaccines for this viral virus still requires a long research in all field studies.
Based on Table 1, favipiravir has a BE value of -4.14 kcal mol-1. This value is higher than native ligand, so this compound is estimated to be weakly constrained to the Mpro receptor relative to a native ligand. China and Japan used this drug to diagnose and treat influenza 52. Favipiravir has not shown a binding effect under 100 µM 21. Recent studies have suggested that favipiravir has been used to treat influenza infection (A, B, C). This drug was also used to treat H5N1, Ebola (EBOV), human norovirus, and human arenavirus 49,53. The inhibition of RNA-dependent polymerase is a mechanism of favipiravir in the healing process 14. The further research in order to obtain more comprehensive data 54,55. Chloroquine sulfate, cefotaxime, salbutamol sulfate, acetaminophen, and acetylcysteine do not show any results that could be considered from BE results.
According to Table 1, the native ligand is well-posed at the binding site of GLU166, CYS145, and GLY143 due to conventional hydrogen bonds. Subsequently, this novel inhibitor also interacts with residues of amino acids in the hydrophobic regions MET165, LEU141, CYS145, HIS41, and LEU27. In addition to hydrogen bond and hydrophobic interaction, the X77 also forms electrostatic interaction through HIS164 to strengthen its position. The existence of a hydrogen bond is crucial to the inhibition mechanism between drug candidates and Mpro receptors. This finding by the authors is compromised by a previous study 56. Almost all molecular docking calculations between ligands and Mpro receptor always react with the amino acid residues of GLY143, next CYS145, GLU166, and HIS163, so the amino acid residues are hypothesized as a priority in inhibiting Mpro receptor 57.
According to BE calculation, nelfinavir is the most potent potential candidate in this study, but this drug was compared to native ligand only via GLU166 for inhibiting the Mpro receptor. Nelfinavir is only attached to MET65 in the hydrophobic region and shows sulfur interaction with CYS145. A conventional hydrogen bond is a primary interaction in this discussion, but the hydrophobic also contributes to the stabilization of the drug-receptor complex 55.
Lopinavir unveils a different interaction with native ligand and interacts with HIS41 via conventional hydrogen bonds. This potential inhibitor binds to MET49, PRO52, ARG188, MET165, and LEU27 in the hydrophobic environment. Sulfur interaction also presents in this complex, CYS145. The previous study showed that this drug was used as an experimental standard. This drug was also successfull in inhibiting HIV, SARS, and MERS treatments 7,36. Lopinavir is used in combination with ritonavir to cure COVID-19 patients in several countries 51. Lopinavir is also co-formulated with ribavirin for an inhibitor of SARS-Cov 36. The routine use of this drug has received a weak recommendation because it does not have sufficient evidence in the case of this pandemic 58. According to the interaction of amino acids, nelfinavir is still considered an excellent potential inhibitor of the Mpro receptor. Beside lopinavir, ligand from vitamin group is regarded as a new potential inhibitor, vitamin D. Vitamin D, an immune system booster, is used to protect COVID-19 patients. It shows hydrogen bond interaction with GLU166 and is useful in agreement with the native ligand. Although it does not show 100% the same interaction relative with the native ligand, with a vitamin D hydrophobic environment to stabilize the complex, namely MET165, HIS41, CYC145, MET49, LEU27, and CYS44. In order to clarify the explanation, we conducted a Pa analysis, Lipinski’s rule, and ligand-protein interaction of potential inhibitors to explore their therapeutic benefits and drug-like properties.
In Pa calculation, umifenovir has specific activity an influenza antiviral. This result is consistent with the previous study that umifenovir was antiviral influenza in Russia and China 19. To contribute, the new potential inhibitor is simulated by an online analysis using the PASS server to identify therapeutic candidates as antiviral agents. According to Table 2, umifenovir, darunavir, oseltamivir, remdesivir, and ribavirin have Pa values between 0.1 to 1. Compounds with an antiviral activity value of Pa in a computational or laboratory analysis 17,18. The Pa value of the PASS analysis results is not specific to SARS-Cov-2. This can be used as a material for futher research consideration. In this result, Pa value nelfinavir has a low antiviral activity score, while oseltamivir shows the highest score.
Lipinski’s rule of five gives us an overview of the drug-like inhibitor candidate. Overall, in Table 2, compounds with the violation value of more than one do not meet the criteria for the drug-likeness 59. The value of MV is a parameter for the penetration of drugs in the human body’s cell membrane. If the MV is more than 500 Da, the drugs hardly enter into the cell membrane. Nelfinavir, lopinavir, ritonavir, baloxivir marboxil, darunavir, cobicistat, and remdesivir have MV greater than 500 Da, and may interfere with the diffusion of the cell membrane. It was also the case for logP, the H-bond donor, and the acceptor. If the limit of Lipinski’s rule of five is violated by a candidate inhibitor, the candidates may not be suitable for laboratory synthesis 60. Lipinski’s rule of five still shows that nelfinavir has good criteria to be a drug candidate for this viral virus.
In Figure 3.a. we can observe the nelfinavir-protein interaction on Homo sapien. Activation mechanism of nelfinavir, e.g., ATP-binding cassette, sub-family B (MDR/TAP), member 1 (ABCB1), while inhibition action of protein cytochrome P450, family 3, subfamily A, polypeptide 4 (CYP3A4); cyclin-dependent kinase 2 (CDK2); cytochrome P450, family 3, subfamily A, polypeptide 5 (CYP3A5); v-akt murine thymoma viral oncogene homolog 1 (AKT1); ATP-binding cassette, sub-family G (WHITE), member 2 (ABCG2); cytochrome P450, family 2, subfamily B, polypeptide 6 (CYP2B6); and heat shock protein 90kDa alpha (cytosolic), class A member 1 (HSP90AA1). The binding action of this drug is CYP34A and ABCB1.
Following to Figure 3.b. lopinavir has ATP-binding cassette, sub-family C (CFTR/MRP), member 2 (ABCC2) with score of 0.726. Then, inhibition action to cytochrome P450, family 3, subfamily A, polypeptide 4 (CYP3A4); zinc metallopeptidase STE24 (ZMPSTE24); and ATP-binding cassette, sub-family B(MDR/TAP), member 11 (ABCB11) with score 0.968; 0.942; 0.700, respectively. Binding action to protein CYP3A4 with score of 0.968. The vitamin D-protein interaction prediction on Figure 3.c. This vitamin shows an activation process to bone gamma-carboxyglutamate (gla) protein (BGLAP); vitamin D (1,25- dihydroxyvitamin D3) receptor (VDR); fibroblast growth factor 23 (FGF23); parathyroid hormone (PTH); cyclin-dependent kinase 2 (CDK2); and klotho (KL) with score 0.996;0.996; 0.800; 0.986; 0.943, and 0.917, respectively. BGLAP, PTH, and CDK2 also experience inhibition route with score 0.786; 0.986; and 0.700, singly. Despite binding activity of this vitamin is on VDR (0.800) and group-specific component (GC, 0.900).
Ritonavir also produces activation, inhibition, and binding pathways prediction on the protein of Homo sapiens, namely activation mechanism on the protein of ATP-binding cassette, sub-family B (MDR/TAP); member 1 (ABCB1), cytochrome P450, family 2, subfamily C, polypeptide 9 (CYP22C9); scavenger receptor class B, member 1 (SCARB1); thrombospondin receptor (CD36); and scavenger receptor class B, member 2 (SCARB2). Protein CYP3A4; ZMPSTE24; CYP3A5; cytochrome P450, family 2, subfamily D, polypeptide 6 (CYP2D6); and caspase 1 (CASP1) are employed an inhibition mode, while CYP3A4 and CYP2C9 predict binding schema (see Figure 3.d.). This pathway prediction is in good agreement with the previous study 61.
{kind=link}