This study investigated the relationship between adipose tissue imaging parameters and the risk of developing ACLF in patients with acute decompensation of cirrhosis. The results indicate that individuals with higher SAT radiodensity are more susceptible to developing ACLF in the context of acute decompensation of cirrhosis(8). This finding introduces a novel predictive factor for ACLF occurrence. Similar associations have also been observed in prognostic studies involving patients with cirrhosis. Therefore, this study proposes SAT radiodensity as a new independent predictive factor for ACLF. Furthermore, a predictive model integrating clinical laboratory examinations and SAT density was developed to identify individuals at higher risk of ACLF among those with acute decompensation of cirrhosis. This model aims to facilitate early clinical intervention and improve patient survival rates.
The pathogenesis of ACLF is exceedingly complex, making it challenging to accurately and comprehensively screen patients at higher risk of occurrence based solely on clinical indicators. Numerous studies have investigated the liver morphological indicators and quantitative parameters of skeletal muscles in patients with cirrhosis to establish predictive models for ACLF occurrence and prognosis(4, 10). However, SAT— an important predictive factor reflecting patient body composition and nutritional status—has not been incorporated in previous predictive models.
Previous studies have indicated that sarcopenia is an independent predictor of mortality in patients with ACLF(10). However, the significance of adipose tissue in ACLF occurrence and progression remains unclear. Total body adipose tissue comprises VAT and SAT, each potentially playing an independent role, necessitating separate investigations of their relationships with ACLF. The radiodensity of adipose tissue can be objectively measured in HU using CT scans. The mean radiodensity of adipose tissue obtained from CT scans has been introduced as an indirect surrogate marker of adipose tissue quality(11). The imaging parameters of SAT obtained from CT scans serve as good indicators for assessing the body composition and nutritional status of patients with acute decompensation of cirrhosis. HU not only represents triglyceride storage in adipose tissue but also includes other aspects of tissue structure, such as water, blood, and residual fat cell components(11).
We believe that SAT, to some extent, reflects the nutritional status of patients with cirrhosis, which is crucial for their ability to withstand disease progression. Unlike BMI, a traditional indicator for assessing body composition, which can be significantly influenced by the general condition of patients, such as the presence of ascites or the use of diuretics(12), adipose tissue parameters obtained from CT scans are not affected by these conditions. Furthermore, patients with cirrhosis typically undergo CT scans, making it convenient to obtain adipose tissue parameters. Additionally, while contrast-enhanced CT scans can also extract adipose tissue parameters, they are unsuitable for patients with acute decompensation of cirrhosis. When measuring SAT density, the values obtained from plain and contrast-enhanced CT scans exhibited high consistency(13). However, contrast-enhanced scans impose a greater financial burden and higher radiation doses on patients.
Previous studies have primarily focused on SAT radiodensity in patients with cirrhosis. For instance, Ebadi et al. reported that patients with cirrhosis had relatively higher SAT radiodensity, which was associated with higher mortality rates. The reshaping of SAT morphology in patients with high SAT radiodensity may indicate reduced fat storage and changes in tissue characteristics(9). In another study, Ebadi et al. demonstrated that a lower SATI was associated with higher mortality rates in female patients with cirrhosis, potentially reflecting the depletion of the body's primary energy reservoir with a good metabolic status, leading to poor clinical outcomes(12). Furthermore, related research in malignancies, such as liver and colon cancer, suggests that SAT radiodensity is associated with disease prognosis(14, 15).
SAT plays a crucial role in lipid storage and energy balance. High SAT radiodensity may reflect severe energy consumption induced by cirrhosis, leading to adverse clinical outcomes. Recent studies have highlighted the comprehensive endocrine functions of adipose tissue, where adipose factors influence the regulation of various metabolic and inflammatory states. The cellular composition of adipose tissue, including adipocytes and macrophages, plays an important role in regulating responses to metabolic states, the release of adipose factors, and potential effects on other tissues(16). Therefore, high SAT radiodensity not only signifies low SAT volume but also indicates adipose tissue remodeling. Its morphological features include small atrophied adipocytes, expanded interstitial spaces, and mononuclear cell infiltration. Moreover, increased SAT radiodensity is associated with a higher risk of decompensation in patients with cirrhosis(17).
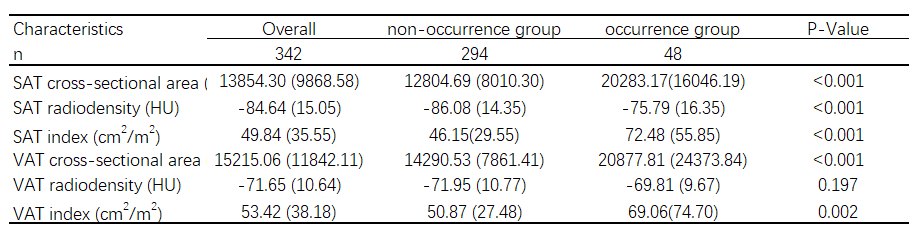
In this study, we delineated two ROIs and examined the influence of SAT and VAT characteristics on the likelihood of ACLF development. Despite conducting quantitative and normalized index analyses of SAT and VAT, no significant results were found. We speculate two plausible reasons for this outcome. First, the small number of patients in the ACLF occurrence group may have led to inconclusive results in the statistical analysis of both variables. Second, existing research has suggested a U-shaped relationship between SATI, VATI, and the prognosis of patients with cirrhosis, in which excessively high or low indices may lead to unfavorable outcomes(18). Hence, we hypothesized that a similar U-shaped relationship exists between these variables and the risk of developing ACLF. Further investigation with larger sample sizes is needed to explore this relationship.
This study also had several limitations. First, previous research on body composition assessment in patients with cirrhosis found that fat depletion was more common in female patients, while muscle depletion was more common in male patients(12, 19). However, in our study, the number of patients in the ACLF occurrence group was insufficient to support subgroup analysis based on sex due to the need to collect patient CT scan data. Second, viral hepatitis was the predominant etiology among the enrolled patients; therefore, future studies should include patients with other etiologies. Lastly, our study was a retrospective cohort study, and further validation of the predictive accuracy of SAT radiodensity for ACLF occurrence in patients with acute decompensation of cirrhosis may be needed in other cohorts or prospective studies.
{kind=link}
{kind=link}