Background
Hypomagnesemia has been correlated with inferior outcomes in patients with large B cell lymphoma (LBCL) undergoing stem cell transplants. As T-cell and myeloid cell dysfunction have been associated with low magnesium conditions, we investigated whether serum magnesium (Mg) levels could predict clinical outcomes in LBCL patients who received chimeric antigen receptor T-cell therapy.
Methods
Patients with LBCL who received axi-cel under the ZUMA-1 trial or as FDA approved therapy at Mayo Clinic were examined. Serum samples were obtained at specified time points and cytokine analysis was performed. Single cell RNA sequencing was performed on peripheral blood mononuclear cells. The Student T-test, Kruskal Wallis, or Fisher's Exact Tests were used to compare differences in demographics across Mg levels. Survival curves were plotted using the Kaplan-Meier methodology and compared using the Wilcoxon test.
Results
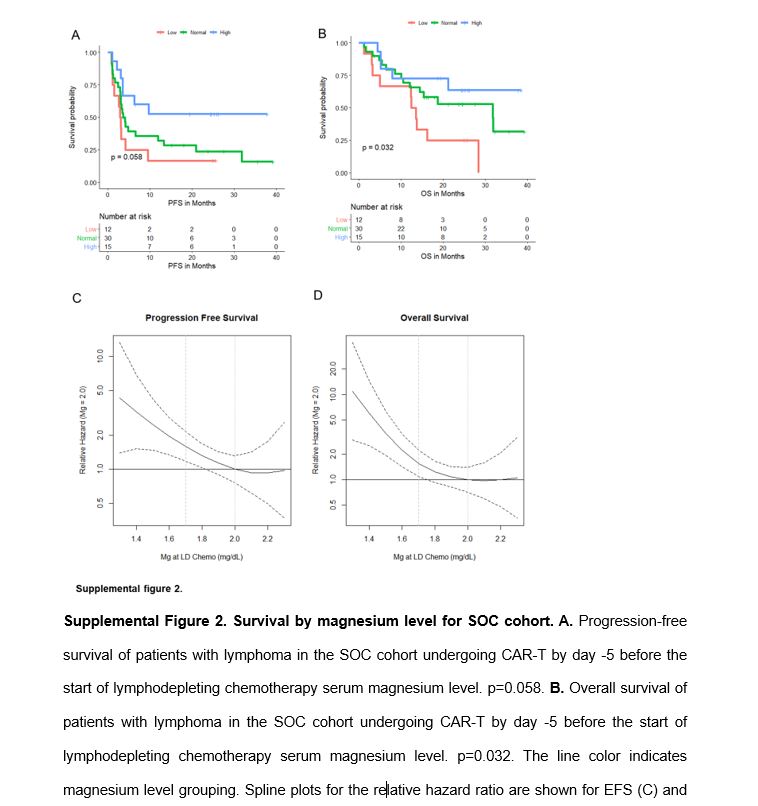
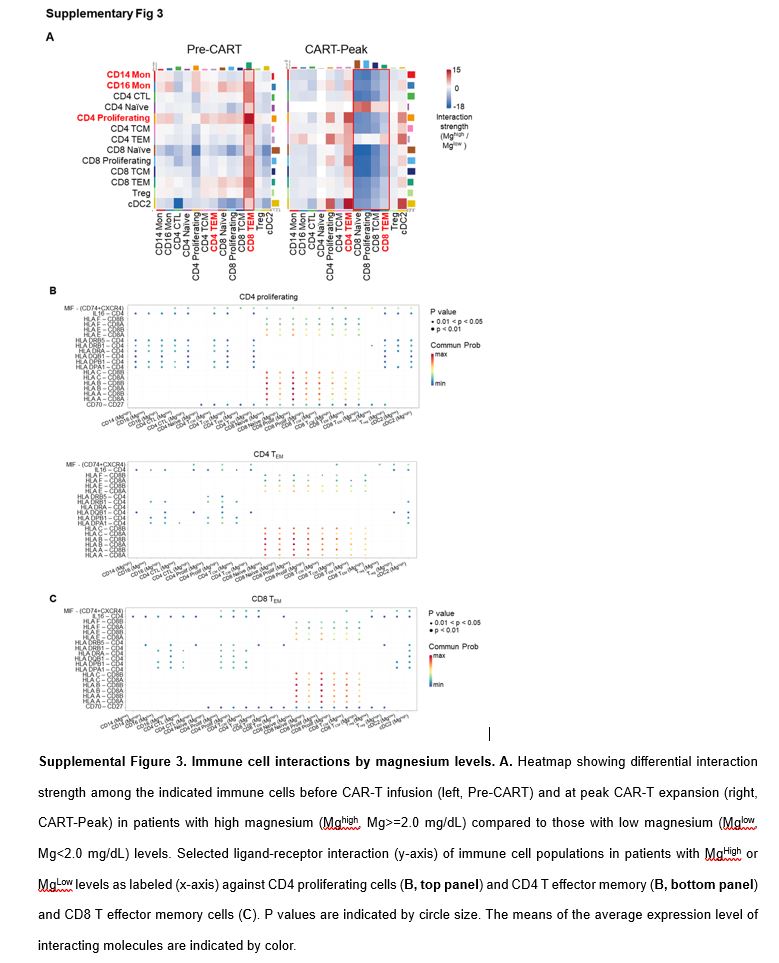
We found that hypomagnesemia before lymphodepletion chemotherapy predicted for inferior progression-free and overall survival in the pivotal study ZUMA-1 (NCT02348216). These results were validated in an independent cohort of LBCL patients receiving axicabtagene ciloleucel (axi-cel) at Mayo Clinic. Hypomagnesemia correlated with increased inflammatory serum markers and cytokine levels including ferritin, IL-6, IL1Ra, IL-8, and MIP1a. scRNAseq analysis unveiled altered immune interactions between monocytes and T cells with a concordant immune suppressive transcriptome.
Conclusions
Hypomagnesemia at the time of CAR-T infusion associates with an unfavorable inflammatory profile and decreased response and survival in LBCL patients receiving axi-cel. These findings suggest a potentially actionable prognostic factor for patients with large cell lymphoma undergoing CAR-T.
{kind=link}
{kind=link}
{kind=link}