mRNA technology holds vast potential for treating a variety of diseases, with the current success of COVID-19 vaccines accelerating the development of mRNA-based drugs.1,2 In cancer therapy, mRNA-based therapies are mainly explored for gene restoration, gene editing, and inducing cells to produce cytokines/antigens that activate/improve immune responses.5 For example, NPs carrying PTEN mRNA have been shown to restore PTEN, a tumor suppressor, thereby inhibiting tumor growth in PTEN null or mutated prostate cancer mouse models.6 Similarly, NPs containing p53 mRNA have reprogrammed the immune tumor microenvironment of hepatocellular carcinoma (HCC) tumors, improving antitumor effects by restoring p53 expression.7 Deletions or mutations in PTEN and/or P53 are observed in 50–80% of the TNBC subtypes and their metastatic cases, indicating significant potential for PTEN and p53 NPs in TNBC therapies.32–34 However, current cancer therapies are often evaluated using cell line-based tumor models, which pose significant challenges for clinical translation due to their lack of predictive value. They fail to retain histologic characteristics, genomic signatures, and tumor heterogeneity of patient tumors, leading to discrepancies between preclinical results and clinical outcomes.21,22 Additionally, TNBC, in particular, is difficult to treat due to its heterogeneity and lack of specific targets, making chemotherapy the primary treatment option, which is associated with drug resistance, CSC enrichment, and tumorigenesis.26
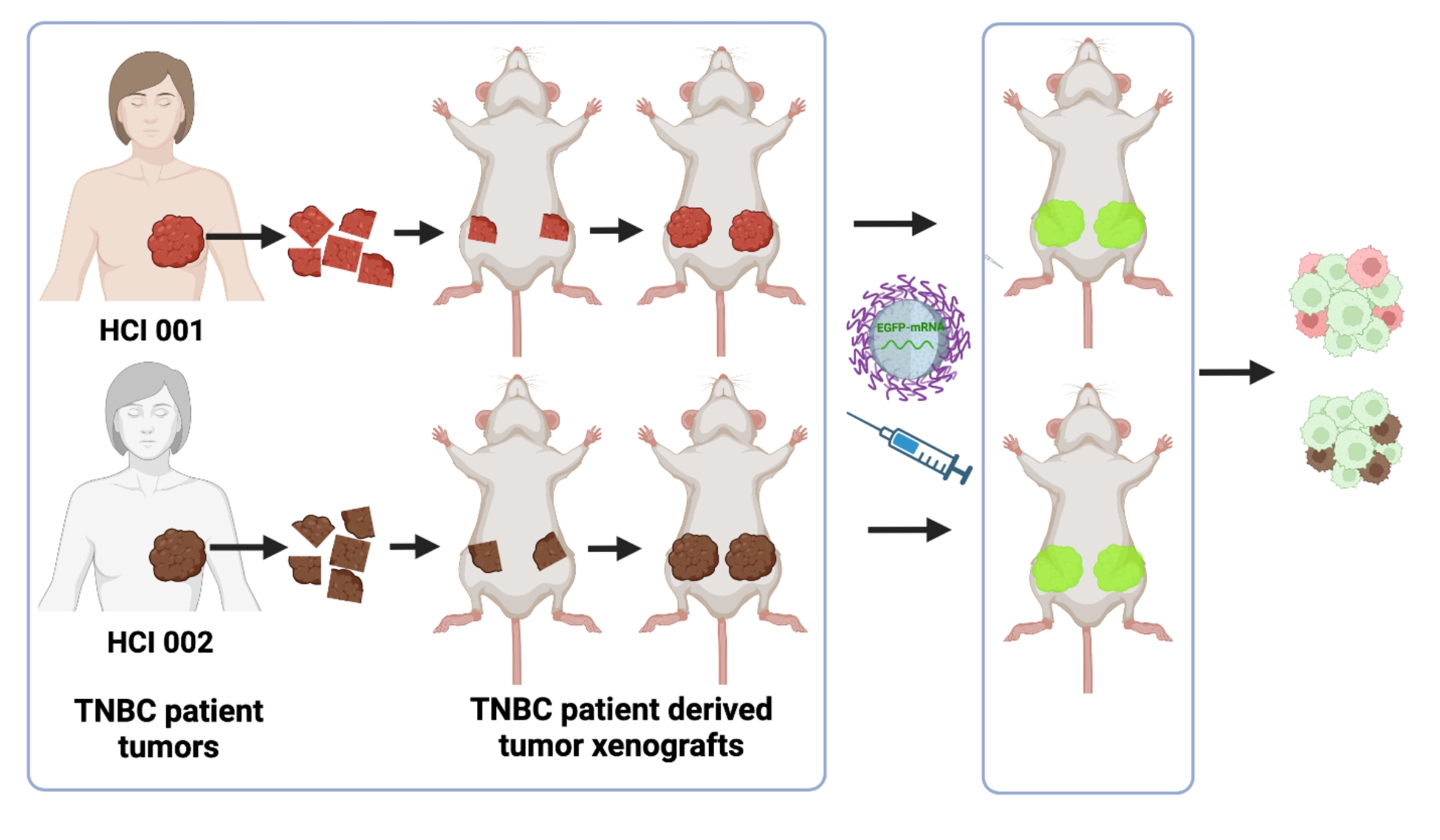
In this context, PDX models represent human tumors’ complexity and heterogeneity, exhibiting high clinical concordance. PDX models are created by surgically implanting patient tumors into immunodeficient mice, preserving tumor microenvironment, heterogeneity, and three-dimensional architecture.23,26 In this study, we demonstrated the effective delivery of mRNA to both mesenchymal MDA-MB-231 and epithelial SUM149 TNBC cell lines, which are typically difficult to transfect. This indicates that our NPs can successfully enter the cells via endocytic pathways, efficiently escape endosomes, and deliver their cargo. We chose two different PDX tumors from 2 patients with varying chemotherapy exposure, resulting in different sensitivity to chemotherapy, as we previously validated.26 Our results demonstrated that NPs could effectively transfect PDX tumors without significant differences in transfection efficiency between the two different PDX tumor models, suggesting that our mRNA-NPs may overcome PDX heterogeneity regardless of chemoresistance or chemosensitivity. Additionally, i.v. administration of mRNA-NPs resulted in effective accumulation in PDX tumors via EPR-related mechanisms, protecting the mRNA from degradation and delivering functional mRNA into tumor cells. These results align with previous studies that demonstrated the efficacy of polymeric NPs for mRNA delivery in cell-line-based prostate and HCC tumor models.2,5,6 However, our study highlights the potential of these NPs in clinically relevant TNBC PDX models. This suggests that our mRNA-NPs platform can be used to deliver therapeutic mRNAs, such as PTEN-mRNA, to PTEN-deficient PDX tumors and/or p53-mRNA to p53-mutated tumors. Such studies involving the evaluation of mRNA-NPs in clinically relevant PDX models can bridge the gap in translating mRNA NPs to clinical applications for cancer therapy.23
PDX tumors represent a heterogeneous tumor microenvironment of human tumors, encompassing various cell populations, including tumor cells, extracellular matrices, and vascular.24,26 While we did achieve efficient delivery of mRNA to PDX tumors overall, further in vivo studies need to be performed to determine if mRNA is delivered differentially between tumor cells, tumor-associated macrophages, and other cell populations.35 It is also important to investigate any differences in mRNA transfection efficiency among the diverse cell populations in two PDX tumor models. The complexity and heterogeneity of TNBC in different patients cannot be fully represented by only two PDX models. Therefore, further testing mRNA delivery efficacy using a broader range of PDX tumors is needed to address this limitation. Nonetheless, the consistent results from two different PDX tumor models in our studies suggest a degree of commonality with significant implications. Additionally, since EGFP-mRNA lacks therapeutic potential, further studies are needed to validate our NPs using therapeutic mRNAs, such as tumor suppressors PTEN and P53, in TNBC PDX models. Furthermore, since our current PDX models use immunocompromised mice, developing TNBC PDX tumors in humanized mouse models for evaluating PTEN/P53 mRNA-NPs will greatly improve the predictive values and advance personalized mRNA nanotherapies towards clinical application.
Although LNP platforms are well studied for mRNA delivery,1 their potential for cancer applications and tumor accumulation remains under explored. In contrast, polymeric NP platforms36 offer versatility with advantages such as controlled and sustained release and stimuli responsiveness, yet their use in mRNA delivery is insufficiently examined. Previously, we showed that polymeric NPs can efficiently accumulate in TNBC PDX tumors.26 In this study, we used simple polymeric NP systems that encapsulated a high mRNA load and successfully transfected TNBC PDX tumors after either intra-tumoral or intravenous administration. These studies indicate that polymeric NPs are effective for mRNA delivery and suitable for cancer applications, opening the doors for exploring a vast range of polymeric mRNA-NP platforms.
{kind=link}