Our present study compared the safety and efficacy of HPSD ablation (50 W) to conventional power (30–35 W) in patients with PAF. In terms of contact force (CF)–sensing catheters and PAF, this retrospective cohort study possessed the relatively large population in this field, and suggested that HPSD ablation saved total procedure time, significantly reduced the exposure to radiation in both operator and patient, and could be performed safely with no additional complications compared to the conventional power group. In terms of the recurrence rate of atrial fibrillation, the results were consistent in both groups.
Radiofrequency catheter ablation was one of the important measures for the treatment of PAF in recent years. Over the past decade, ablation success rates had increased with advancements in ablation techniques, especially after the introduction of contact force–sensing catheters. The mechanism of RF ablation was intricate, in which RF energy heating consists of two stages, the early resistive heating stage and the later conductive heating stage, while conductive heating was generally considered to cause deeper collateral damage. Compared to conventional power catheter ablation, HPSD-RFA was believed to damage tissues by resistive heating and can minimize the endocardial retention that may occur in an irrigated tip catheter heated at lower power5.
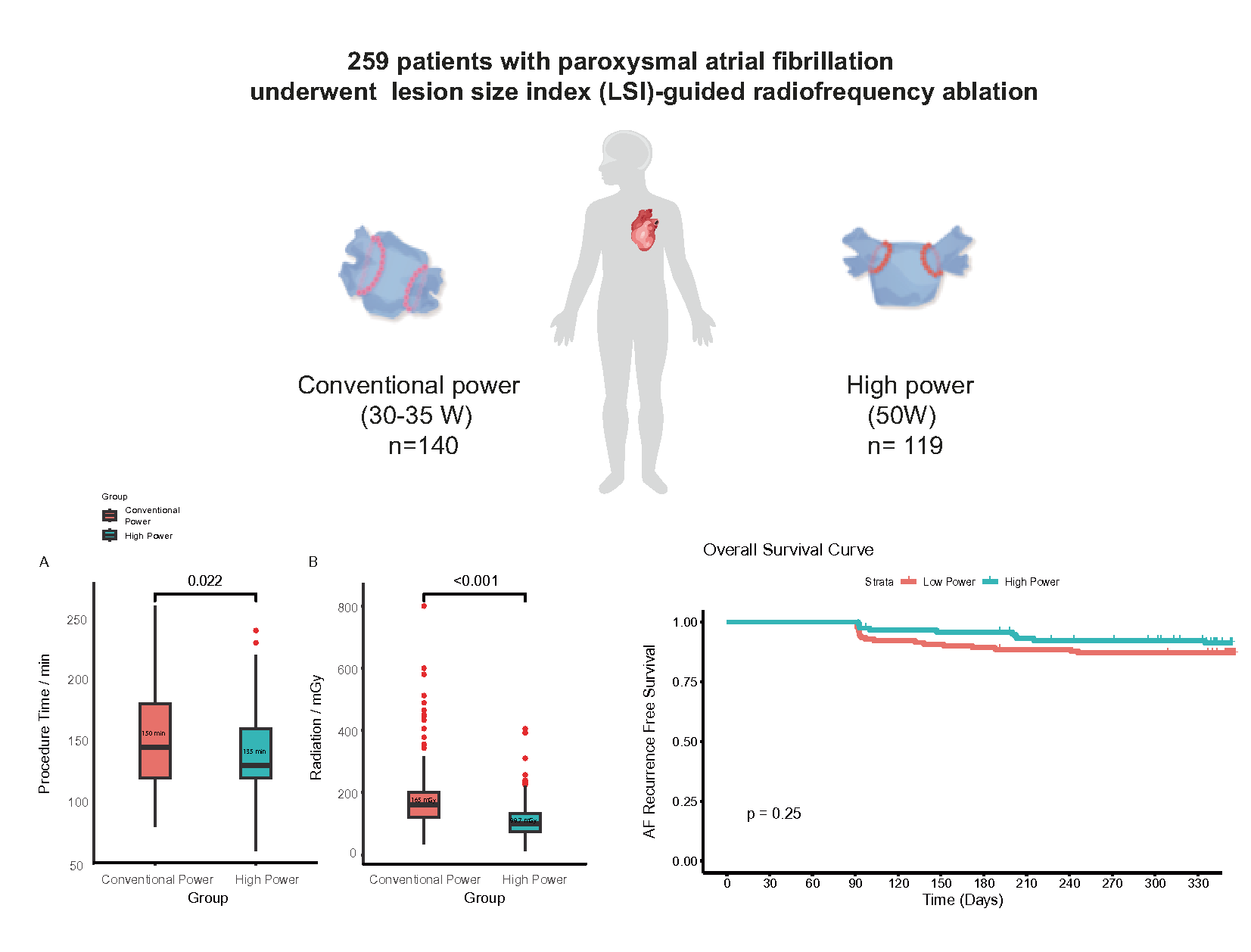
The high-power RF energy from the small electrodes heated the tissue immediately and rapidly by producing a high current12. Based on the above situation, previous studies had consistently shown a shorter procedure time for HPSD-RFA13. Our study also demonstrated that the total operative time was significantly reduced in the HPSD group. A clear advantage of HPSD-RFA was revealed in our current study in reducing the time of intravenous fluid infusion and anesthesia by shortening the procedure time. Some studies had reported a statistically significant reduction in fluoroscopy time for HPSD-RFA, but others showed no difference10. Although the effect on fluoroscopy time was inconsistent in previous studies, our results suggested that HPSD could significantly reduce the exposure to radiation, which had a direct beneficial effect on the patient, operator and supporting personnel.
A prospective randomized controlled trial showed that HPSD ablation reduced the procedure time and also decreased the number of ablation lesions for PVI without increasing the incidence of complications14. HPSD ablation had also been shown to reduce the incidence of gaps between ablation sites and reduced the risk of atrial perforation caused by excessive transmural ablation15. Studies on HPSD that had been carried out in AF patients indicated that a catheter radiofrequency ablation power of 45 ~ 50 W was safe and effective8,16. Our data also showed that HPSD had a relatively low incidence of complications, including no thromboembolic complications, pericardial tamponade and atrio-esophageal fistula, which was consistent with previous research. However, pulmonary vein reconnection following PVI remains a major clinical challenge. Using in vitro and in vivo models, Bhaskaran et al. demonstrated that, compared to the LPLD ablations, the lesion widths were similar and the lesion depths were shallower for the HPSD 50 W and 60 W ablations17. There was concern that the shallower lesions associated with HPSD may cause a higher recurrence rate of late arrhythmia compared to conventional power12. We therefore observed the clinical outcomes of LSI-guided HPSD ablation at 12 months of follow-up and suggested that the 50 W group had a similar rate of being arrhythmia-free at 12 months compared to the conventional power group. It was worth mentioning that, we found that HPSD had a better prognosis for women with PAF, with a lower recurrence rate after ablation at 1 year follow-up, although there was no statistical difference compared to LPSD. Therefore, our existing data suggests that HPSD ablation is suitable for treating PAF in both males and females.
In general, our present study showed that HPSD-RFA was a safe and effective strategy for the treatment of patients with PAF. It was still necessary to include more patients with PAF and longer follow-up to determine the advantages of HPSD-RFA.
Study limitations
First, this study was a retrospective cohort, and patients were not prospectively recruited, but were sequentially selected. Second, Secondary pulmonary vein potential mapping was not performed in enrolled patients to reflect the recovery of pulmonary vein potential. Third, ablation parameters, including contact force, force–time-integral, and continuity (distance between adjacent ablation sites), were not compared between the two groups. We were unable to assess subclinical esophageal injury because routine esophageal endoscopy monitoring was not implemented in our study. Finally, systematic monitoring for recurrences after ablation was also required in future studies.
{kind=link}