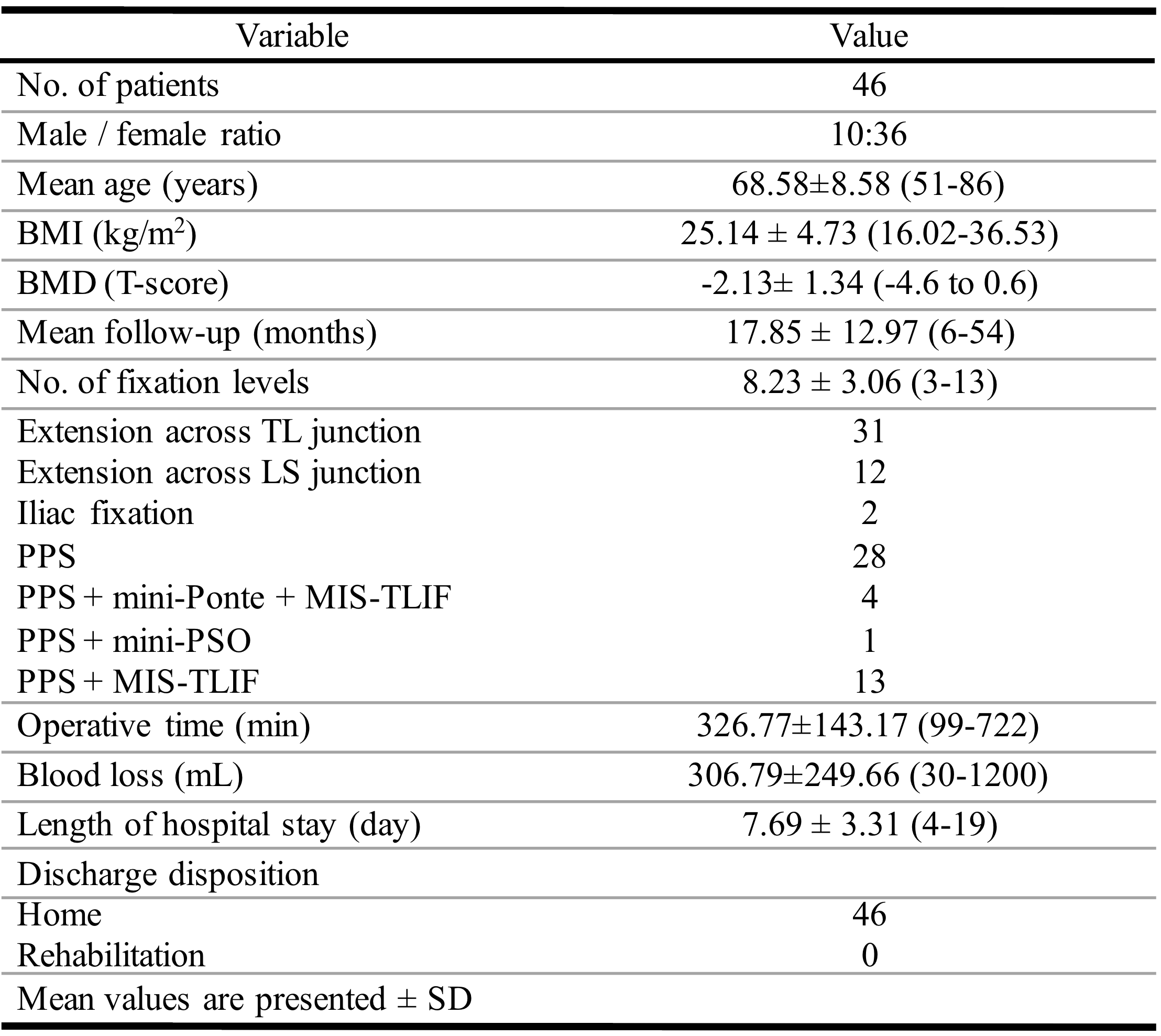
MIS has garnered significant attention and acceptance, particularly in recent decades, for its effectiveness in treating degenerative spinal diseases. In our study, employing posterior MIS on 46 patients have consistently shown that MIS techniques offer substantial benefits for ASD. These advantages include restoring sagittal balance and the coronal plane while simultaneously reducing major surgical complications, with notably lower reoperation rates observed in MIS patients. The positive impact on patients' quality of life is evident across various clinical settings, mirroring findings from traditional open ASD surgery and MIS procedures. [23–25] Among our patients, in addition to achieving good radiographic outcomes, most reported high satisfaction after surgery. The mean ODI and VAS scores between baseline and last follow-up for back pain decreased from 34.9 to 23.6 (resulting in a 32.3% decrease) and from 8.4 to 3.4 (resulting in a 59.5% decrease), respectively. These findings demonstrate patients with adult spinal deformity after posterior MIS surgery achieve satisfactory daily living activities in comparison with preoperative levels.
Currently, the surgical treatment for adult spinal deformities involves an anterior procedure followed by posterior instrumentation and fusion. The circumferential approach has been considered necessary to enhance deformity correction especially in kyphosis correction. [26] However, compared to circumferential MIS or the anterior approach, many articles also mention the favorable outcomes of the posterior-only MIS approach. A study illustrated that using a posterior-only approach for the treatment of degenerative lumbar scoliosis, kyphosis, or both combined with spondylolisthesis showed an improved positive correlation between the increase in JOA score and the increase in the lumbar lordosis angle.[27] Kim et al.'s published study demonstrated that posterior segmental spinal instrumentation and fusion without anterior apical release of lumbar curves resulted in superior total SRS scores, comparable complication rates, and analogous radiographic parameters. [28] Verde et al. conducted both double-route and isolated posterior-route procedures, achieving significant corrections in both approaches. [29] Good et al. proposed that single-way access is effective in correcting moderate and severe curves, potentially reducing the side effects associated with the double approach.[30]
Compared to anterior or circumferential approaches, the posterior only approach provides several advantages. Firstly, the posterior only approach offers the convenience of a single-stage procedure performed in a single position, eliminating the need to reposition the patient, which is a source of increased surgical time and potentially patient risk correlation with anesthesia. Secondly, the surgical technique outlined in this study combines posterior decompression and correction, optionally supplemented with other decompression methods such as TLIF, PONTE, and PSO, as necessary. Thirdly, unlike anterior fusion, which carries risks of injuring major vessels and abdominal organs, posterior procedure only minimizes the likelihood of damaging intra-abdominal structures.
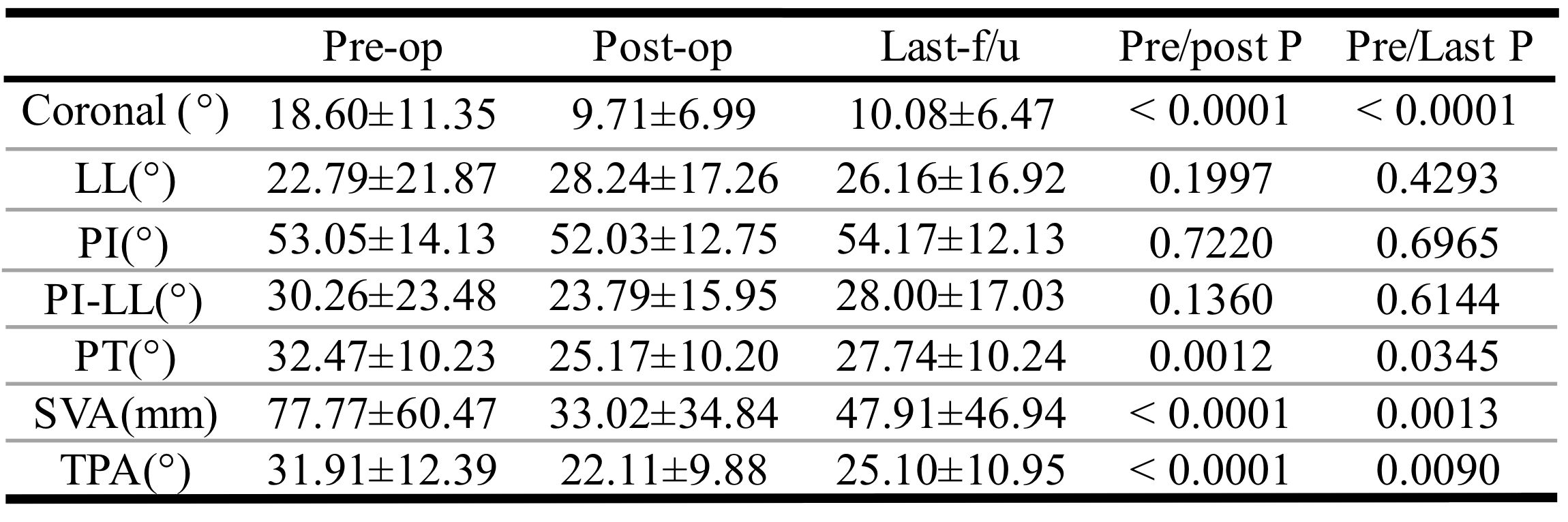
Despite the effectiveness of MIS techniques in addressing degenerative pathologies and their evident advantages over open approaches, there are still face challenging. For patients requiring extensive fusions into the thoracic spine or those with prior instrumentation or individuals with coronal deformities exceeding 20°may not be suitable candidates for MIS techniques. [31–32] Eastlack et al. found that patients selected for MIS had smaller coronal deformity correction compared to those eventually offered open surgery. [33] However, our surgical results demonstrate that the posterior MIS procedure provides a straight forward method for correcting not only improvement of SVA but also coronal deformities. Anand et al. with similar reported significant correction of the Cobb's angle from 18.93° to 6.19° through minimally invasive multilevel percutaneous screw fixation. [34] In our study, a retrospective review of radiographs revealed a notable improvement resulting in a 45.8% decrease in the Cobb's angle (from 18.60 to 10.08). This outcome demonstrates that the posterior MIS approach only can similarly achieve the correction of coronal angle.
In our study, utilizing the posterior MIS approach, significant improvements (P-value < 0.05) were observed not only in the coronal angle but also PT, TPA, and SVA after surgery. Kumar et al. published that lateral access MIS (OLIF and PPS) for adult spinal deformity revealed preoperatively, the measurement of initial SVA was 96.5 mm and improved to 24.1 mm postoperatively. [35] Another study, Park et al. revealed the circumferential MIS approach for treating ASD, demonstrating that it led to an improvement of 3.0° in LL and an increase of 2.1 mm in the SVA, and a decrease of 2.2° in PI-LL. [36] Compared to our results from studies involving lateral access or circumferential MIS, the single-stage posterior MIS approach also achieves excellent corrective effects. Particularly noteworthy is the substantial improvement in SVA, decreasing from 78 mm preoperatively to 33 mm postoperatively (resulting in a 57.7% decrease), indicating remarkable improvement. This is further supported by our statistical analysis of surgical outcomes, providing strong confirmation.
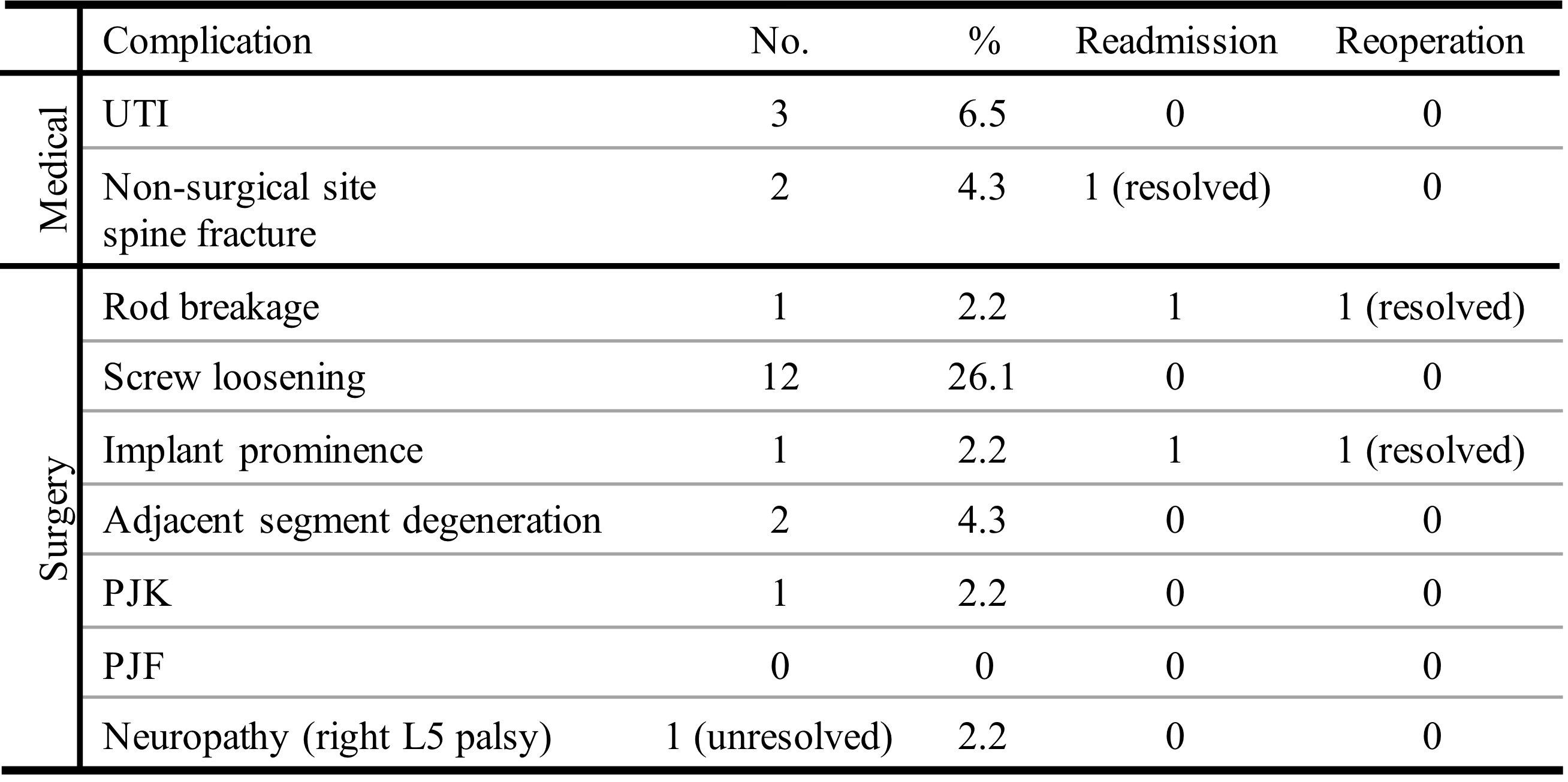
The complication was higher in ASD surgery, especially in the cases need with aggressive deformity correction. Traditional open surgery, exemplified by osteotomy, is effective in restoring sagittal balance but is prone to various complications, including excessive blood loss, neurological deficits, and pseudoarthrosis. [37] In our surgical outcomes, 18 patients experienced surgical complications, accounting for 39.1% of the patient population. Although the complication rate appears high, most cases were only identified through radiographic findings. Specifically, the majority of cases involve asymptomatic (69.6%) or mild pain with low reoperation rate 4.3% for revision surgery. Compared to traditional open surgery, which is associated with relatively high perioperative and postoperative complication rates and medical complications following surgery range from 35–40%, and the reoperation rate varies between 10–50%. [38–40] Regarding the MIS, the diverse nature of approaches such as LLIF, TLIF, PPS, OLIF, etc., introduces considerable variation and contributes to the occurrence of different types of complications. Chan et al. reported that those undergoing cMIS had fewer overall complications compared to hybrid techniques (p = 0.006). [41] Sleiman et al. found that while both the combined approach and the posterior-only approach had similar complication rates [42]
Regarding the reoperation rate, Scheer et al. reported that data collected from a multicenter adult spinal deformity database show an overall reoperation rate of 17% among those who underwent open surgery. [43] Another study published by Hamilton et al. reported an 11% revision rate for MIS, including lumbar interbody fusion (LIF) or transforaminal lumbar interbody fusion (TLIF), and percutaneous pedicle instrumentation. [44] Compared to our statistics, only two individuals, accounting for 4.3%, required reoperation, have similar outcomes compared to other posterior-MIS surgery.
Our study affirms the effectiveness of a posterior-only approach combined minimally invasive procedure, demonstrating satisfactory clinical outcomes. Despite facing surgery-related complications, such as screws loosening, rod breakage and PJK, the technique proves advantageous in correcting overall sagittal and coronal balance. Furthermore, it boasts benefits, including minimal muscle damage, a low risk of nerve injury, minimal bleeding, prompt post-operative recovery, and high patient satisfaction. [45] Utilization of a posterior-only minimally invasive approach as a secure and effective strategy for managing ASD, and decrease revision surgery rate. With the ongoing utilization of MIS surgery for spinal deformities, the inclusion of more patients in future prospective studies will enhance the consolidation and corroboration of the results of this study.
Limitation
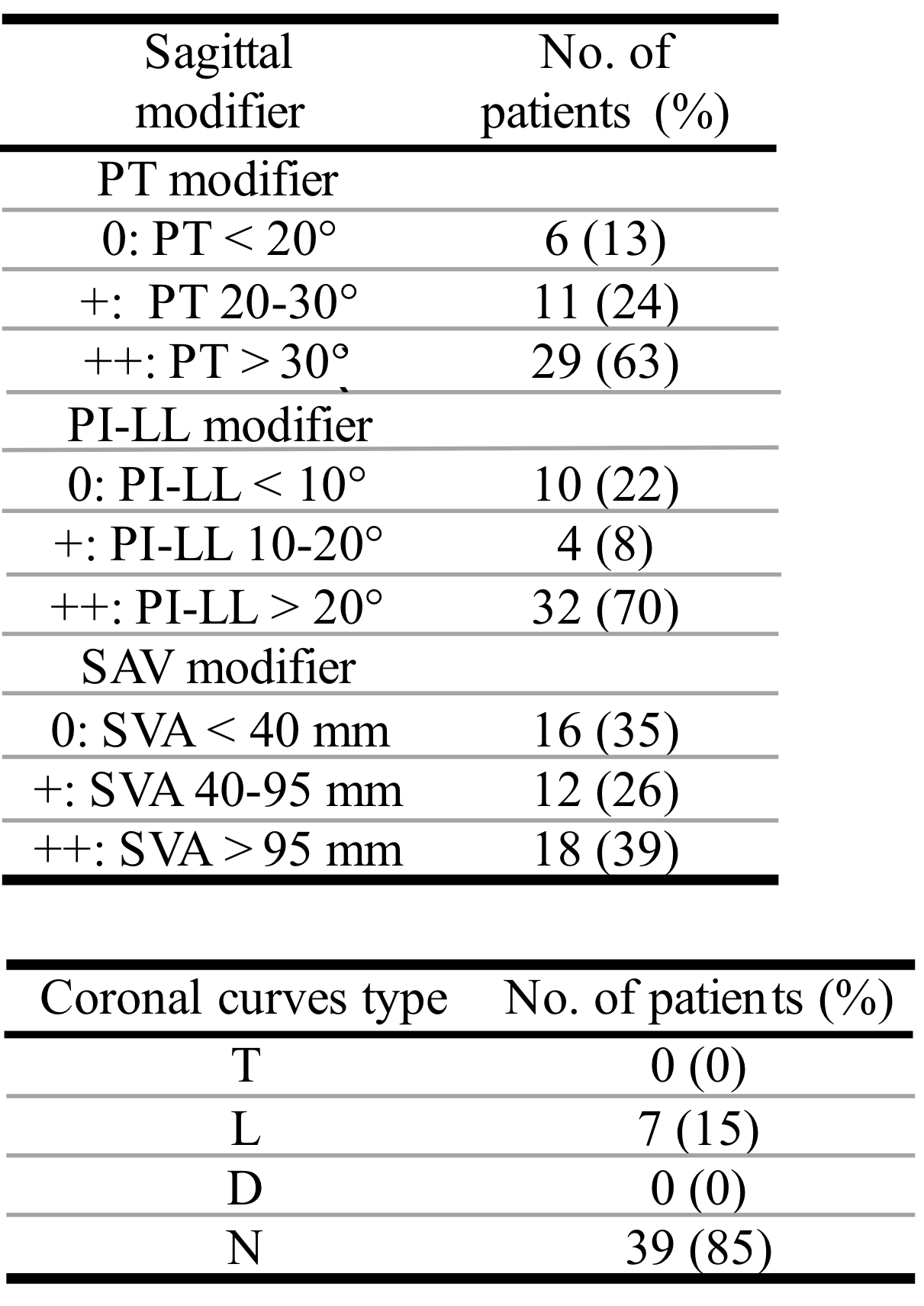
There are several limitations to the study. Firstly, it lacks relatively long-term follow-up results. The majority of patients were followed up for six months to five years, lacking sufficient data for a long-term analysis. Since the pattern of early functional improvement, followed by maximal benefit, and then a slight decline, is observed in many interventions for degenerative pathologies. [46] Secondly, this study represents a case series without a comparator, either a younger group of patients undergoing MIS or patients of all ages undergoing open surgery. A relatively small number of patients and common biases associated with retrospective studies, such as selection and reporting biases, were also observed. Thirdly, this study categorized complications based on the classification proposed by the Klineberg et al., ISSG-AO ASD spine complications classification system, making it comparable only with other studies using this classification. Fourthly, the majority of patients are concentrated in the N/L type of coronal curve. However, for T type patients, further data are needed to ascertain the feasibility of utilizing Ponte or performing PSO procedures.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}