Study design and participants
The protocol and study design of the CABC trial has been fully described previously [36].
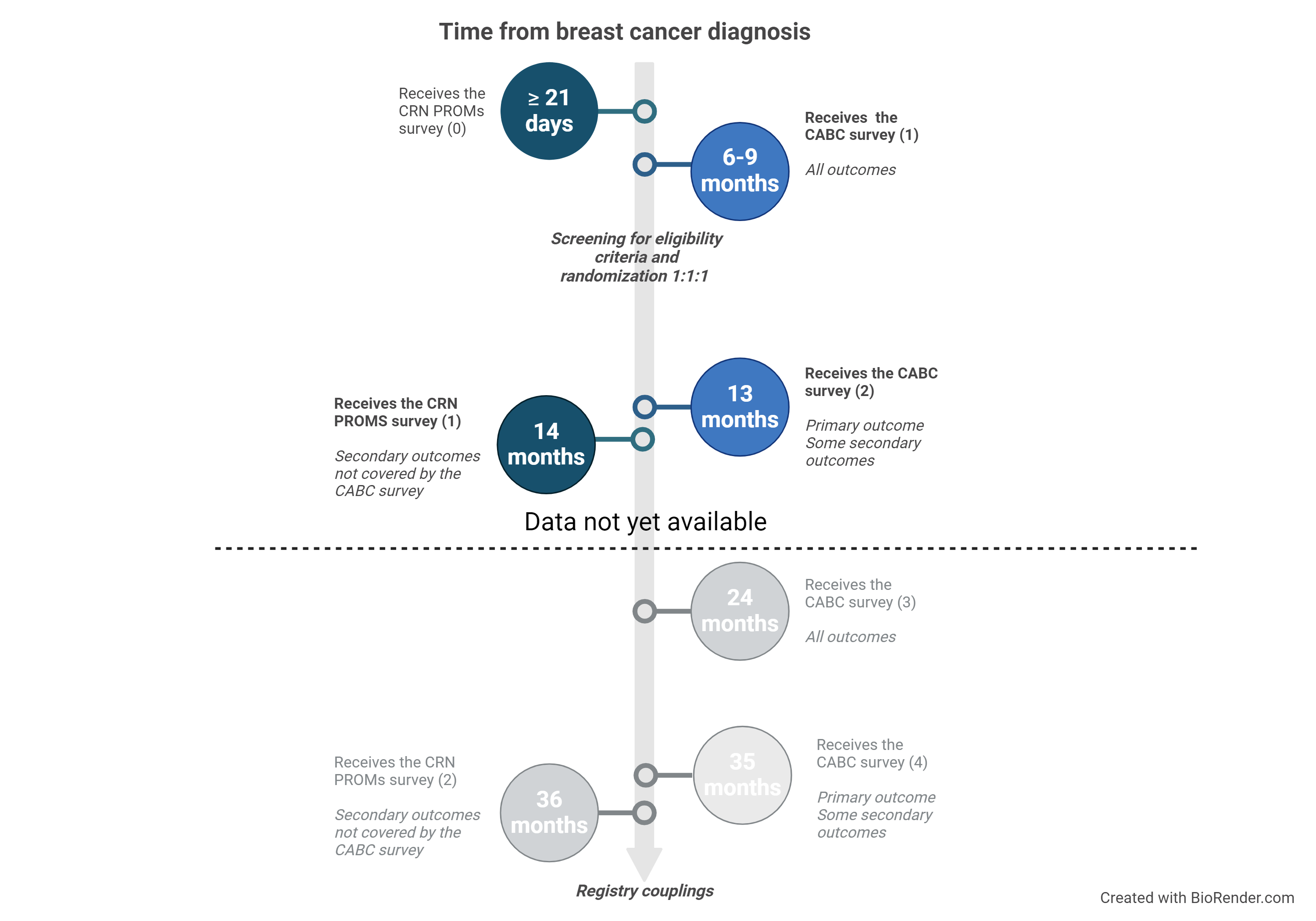
Women diagnosed with either ductal carcinoma in situ, or breast cancer stage I-III, human epidermal growth factor receptor 2–positive (HER2-positive) or estrogen receptor–negative tumor(s)) (ER-negative) registered in the Cancer Registry of Norway (CRN), aged 21–69 years who had completed the digital CRN patient reported outcome measures (CRN PROMs) survey sent to all breast cancer patients at least 21 days following diagnosis [37] were eligible for trial inclusion.
In total 1123 potentially eligible breast cancer patients were identified from the CRN PROMs survey and received the CABC trial specific survey 6–9 months following their diagnosis and in the period January 2021 and May 2023. In total 467 completed the CABC survey which constituted consent and were randomized 1:1:1 to CBI, MBI or usual-care controls. The randomization was concealed, and we employed a block randomization variant without stratification, with block sizes varying between 12 and 27. Twenty-three participants were included in a pilot study and thus excluded from the current study [36].
In an initial, introductory call to participants in the intervention groups, three additional eligibility criteria were assessed: Whether the participants; 1) understood Norwegian, 2) had access to a smartphone or tablet, and 3) had/ were willing to enable phone locks on their devices (a necessity for accessing the app). In total 430 satisfied the eligibility criteria and participants randomized to CBI (n = 140) or MBI (n = 143) accessed the interventions (downloaded the StressProffen app with intervention specific content on their phones with guidance from study staff), whereas participants randomized to controls (n = 147) received no more follow-up (Fig. 1).
CRN PROMs; Cancer Registry of Norway (CRN) patient reported outcome measures (survey sent to all digitally active breast cancer patients after diagnosis). CABC; Coping After Breast Cancer. CBI; cognitive behavioral therapy intervention. MBI; mindfulness-based intervention.
Intervention arms and delivery model
The CBI and MBI interventions, originating from the original StressProffen program (i.e., primarily CBT based but with aspects of mindfulness), were developed to be almost identical in length, design, format and layout, for details see [38]. Each intervention consisted of 10 modules with 9–16 brief steps containing various stress-management related educational material and exercises (i.e., diaphragmatic breathing, visualization, focus) available through text, audio, video, and illustrations. The interventions are self-guided with a 3-day mandatory pause between modules to encourage reflection and practice. The titles of the 10 modules in both interventions are displayed in Supplementary file 1. Examples of CBI and MBI content are displayed in Supplementary file 2 and 3, respectively.
The original StressProffen program was delivered in a simple blended care model (i.e., one in-person introduction session providing rationale for the stress-management concept and guidance in downloading the app, followed by two follow-up phone calls) [33, 34]. Most “health apps” are however downloaded individually from online stores, and are rarely delivered with additional support [39]. The current CABC trial therefore opted to deliver the StressProffen CBI and MBI versions in a digital download-only delivery model. To add a follow-up aspect for the intervention (i.e., to encourage use and adherence), participants were contacted by phone three times during the intervention period (about 1-, 3- and 6-weeks post app access). These follow-up phone calls, although brief, were conducted to ask about status, help resolve any potential technical issues or barriers for use, and through such help motivate continued usage of the app.
Data collection and outcome measures
All outcomes were assessed with the CABC 1 survey at baseline (6–9 months after diagnosis) and with the CABC 2 survey 6 months after baseline (about 13 months after diagnosis). However, since fatigue was already scheduled to be assessed with the ongoing CRN PROMs 2 survey 14 months after diagnosis, this outcome was not included in the CABC 2 survey [36] (Supplementary file 4).
Outcome measures
Primary outcome
The primary outcome, perceived stress, was assessed using Cohen’s 10-item Perceived Stress Scale [40]. Items were rated on a 5-point Likert scale ranging from “never” (0) to “very often (5)” over the last month, and a total score was calculated (0–40). Score 0–13 represents low perceived stress level, 14–26 moderate, and 27–40 high perceived stress level [40].
Secondary outcomes
An anxiety and depression score was generated from four individual items in the brief version of the Patient Health Questionnaire for Depression and Anxiety (PHQ4)[41]. Fatigue was measured using Chalder’s Fatigue Scale (13 items) and presented as a summary score [42]. HRQoL was measured by the RAND Corporation 36-Item Short Form Health Survey (RAND-36). RAND-36 assesses 8 health domains: physical functioning, role limitations caused by physical health problems, role limitations caused by emotional problems, social functioning, emotional well-being, energy/fatigue, pain, and general health perceptions [43]. Mindfulness was assessed using the 15 items from Baer’s 5 Facet Mindfulness Questionnaire (FFMQ-15) and presented as a total score [44, 45]. Coping, helplessness and hopelessness were measured by the Theoretically Originated Measure of the Cognitive Activation Theory of Stress [46]. Sleep (duration and quality) was measured by items from the Norwegian Shift Work, Sleep and Health survey [47]. Rationale and more details on outcome measures are provided in the protocol paper[36]
Sociodemographic and medical data
Sociodemographic data (i.e., age, educational level, relationship and family status, income, physical activity level, smoking and alcohol habits, height, and weight) were obtained from the CRN PROMs 1 survey (administered ≥ 21 days following diagnosis). Medical data on breast cancer diagnosis were obtained from the CRN.
App use
Data related to program use (i.e., such as app progress/activity, time spent using the app, days from first to last use, number of completed modules, etc.) were automatically extracted from user logs that were collected and stored on a secure research server at the Services for Sensitive Data, University of Oslo.
Statistical analysis
All analysis followed a statistical analysis plan that was evaluated by the CABC main project group prior to analysis.
The study was powered to find significant differences in the primary outcome (i.e., 6-month between-group difference in perceived stress) using independent sample t tests. Presumed effect size and variance were based on previous results from the StressProffen study [33, 48]. Originally, we used an alpha level of 5%, but since we had two intervention groups, we needed to adjust for multiple comparisons (two intervention groups) and reduced the alpha level to 2.5% in February 2022. Simultaneously, we downgraded one of the two primary outcomes (HRQoL) to a secondary outcome. Assuming a completion rate of 70%, we needed minimum 335 participants [36], and ended up including 430 participants.
Results for all outcomes were presented as the mean change from baseline to 6-month follow-up, adjusted for baseline values. Between-group differences were calculated as the intervention group changes from baseline minus control group change from baseline. Analyses were performed according to the intention-to-treat principle, with all participants included regardless of app use and loss to follow-up. Missing data on outcomes at baseline and follow-up were imputed using fully conditional specification. In addition, the results from the complete case analysis are presented in Supplementary file 5. Groups were also compared after controlling for the a-priori defined potential confounders of age (grouped as 18–44, 45–54, 55–69), educational level (low and high), having children < 18 years (yes/no), BMI (under- and normal weight, overweight or obese), cancer stage (DCIS + stage 1, stage 2 and 3 or missing) and alcohol use in multivariable regression analyses. Results from these analyses are presented in Supplementary file 6.
For the primary outcome, exploratory subgroup analyses were performed by app completion (completed 0–6 modules vs. 7–10 modules) [34], and perceived stress at baseline[(low vs. moderate/high (due to few individuals in the high group)] and below vs. above median baseline level). P-values are reported for the interactions between subgroup and intervention group to assess whether intervention effects varied by subgroup.
Multiple imputations
Missing data (including due to deaths [n = 2]) on all primary and secondary outcomes at baseline and at follow-up were addressed using multiple imputation by chained equations under the missing-at-random assumption. Each outcome was imputed separately, stratified by randomized group, with all the variables in the multivariable regression model included in the conditional models. Additionally, the EORTC QLQ-C30 emotional functioning scale [49] from CRN PROMs survey 1 and 2 were included as auxiliary variables due to strong association with non-response on CABC survey 2. This was done to satisfy the missing-at-random assumption and reduce the variance of the imputations [50]. To reduce the complexity of the imputation models, the cross-lagged predictors from the surveys were not included in the conditional distributions [51].
For the primary outcome, the imputation models were validated by comparing observed and imputed data, and performing posterior predictive checking of the estimated intervention effect [52]. Since the pattern of missingness was similar for all outcomes, this was not repeated for the secondary outcomes. A total of 100 imputed datasets were created, and the estimates of the intervention effect were combined using Rubin’s rules.
{kind=link}