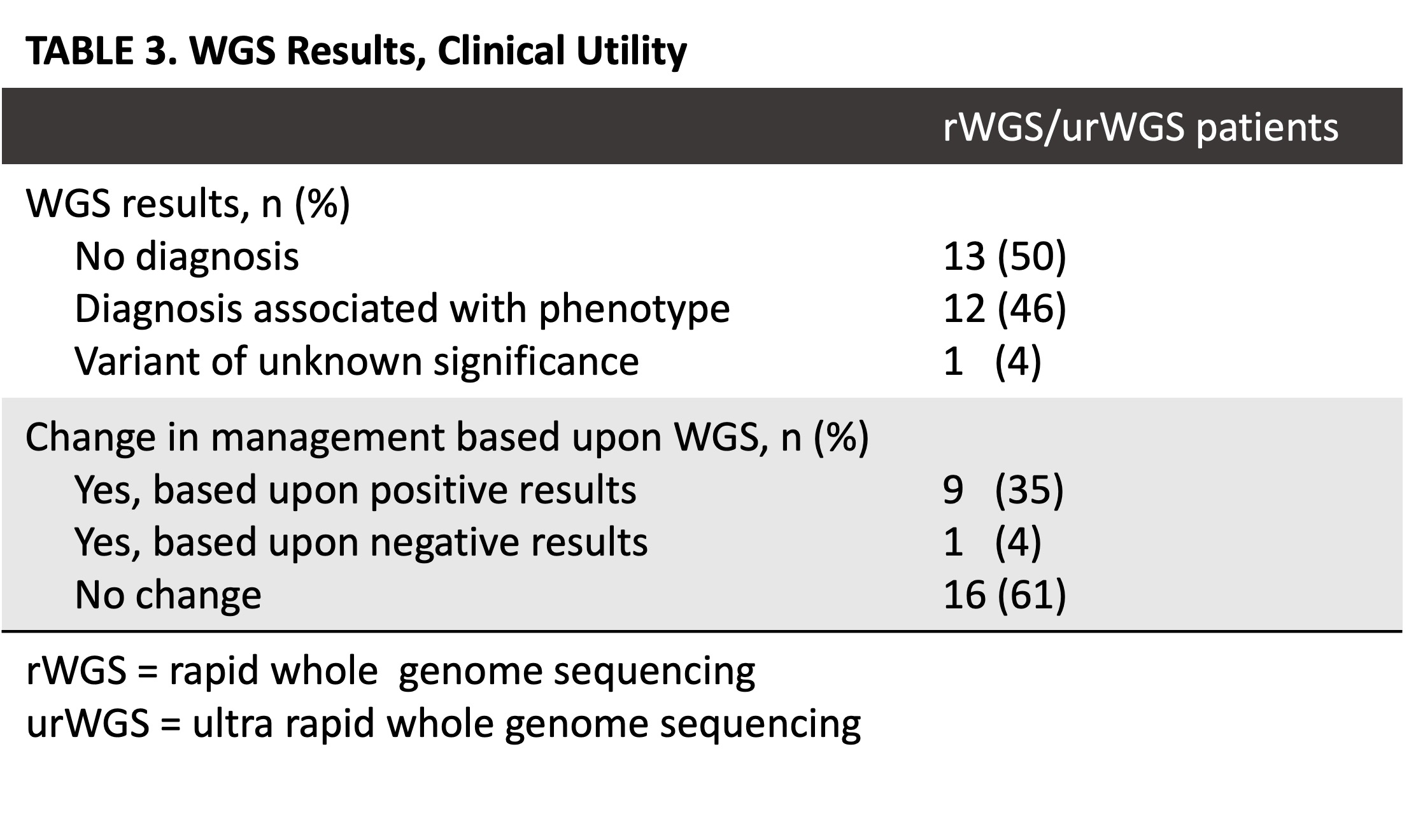
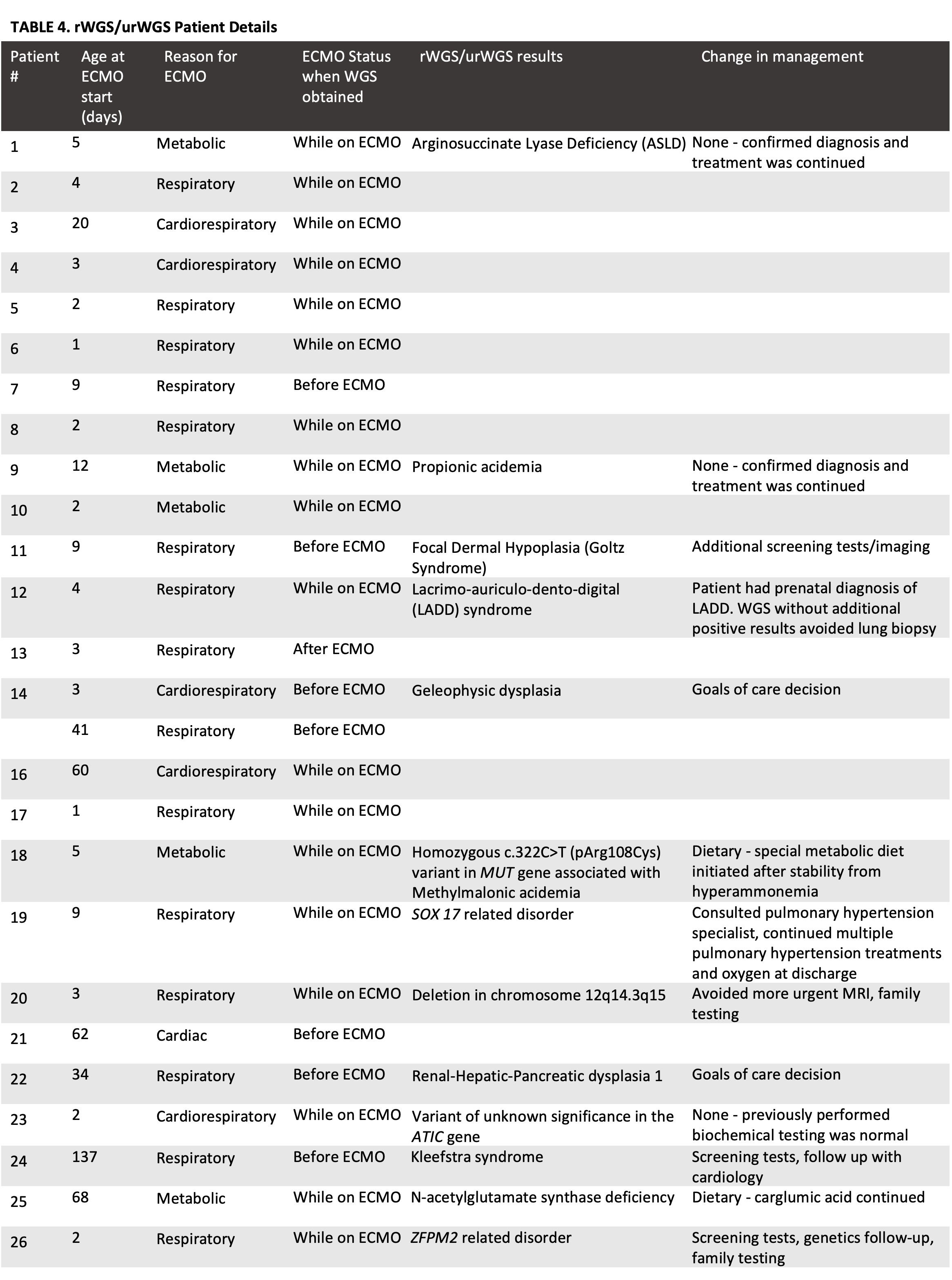
Our study demonstrates that NICU patients requiring ECMO may benefit from rWGS/urWGS with results showing both a high diagnostic rate and clinical utility. The diagnostic rate of 46% in our study follows trends seen in previous studies assessing the use of WGS in cohorts of critically ill infants (3, 15). These previous studies, which have included cohorts with patients with neurodevelopmental disorders and patients critically ill in both the neonatal and pediatric intensive care units, have shown that rWGS/urWGS provides increased diagnosis at improved speed compared to standard genetic testing (3, 7, 15). Additionally, rWGS/urWGS has been shown to impact clinical management (3, 9, 16). The clinical impact resulting from rWGS/urWGS fits into six major categories – no change, dietary/medication changes, additional screening tests, avoidance of tests or invasive procedures, sub-specialty consultation, and decisions regarding goals of care (Table 4). One case, “Patient 12,” had a change in clinical management based on a negative rWGS/urWGS result. This patient had been prenatally diagnosed with lacrimo-auriculo‐dento‐digital (LADD) syndrome. Genomic testing was obtained to rule out other genetic disorders given the severity of the patient’s illness. The negative rWGS, aside from the already known LADD syndrome, resulted in the avoidance of a lung biopsy in this case.
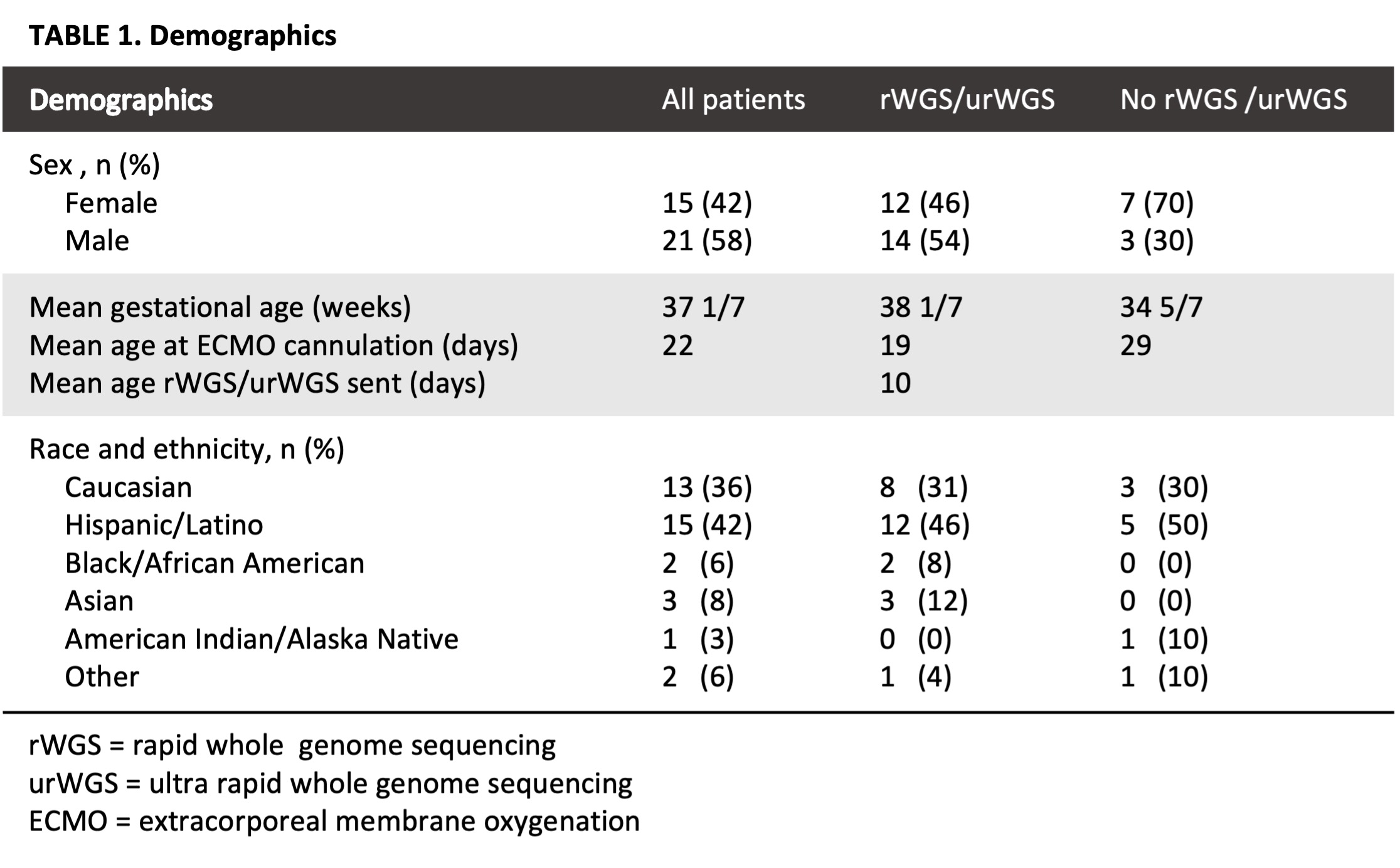
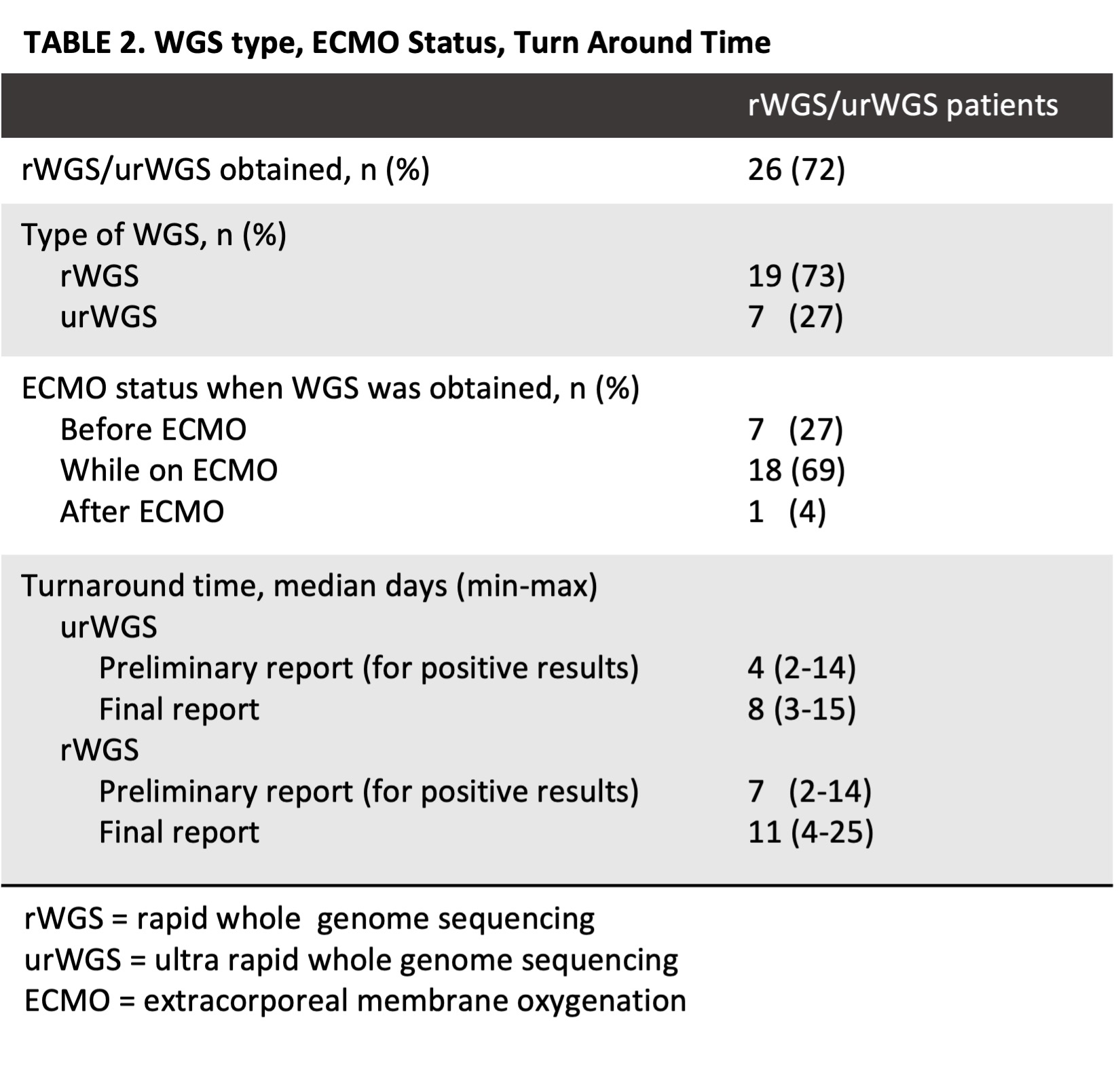
There has been concern about the quality of samples used for genetic testing after blood transfusions (17). It has been shown that DNA from leukoreduced blood products is unlikely to interfere in genetic testing of immunocompetent patients, though there are few studies in the neonatal population (17). Given our population, 18 of the 26 rWGS/urWGS tests (69%) were obtained while on ECMO. Obtaining genetic testing while on ECMO did not appear to affect either the results or clinical utility of rWGS/urWGS in this cohort.
Limitations of the study include that at our institute ECMO is utilized to treat severe neonatal hyperammonemia due to increased availability compared to hemodialysis. Given the genetic basis of many of the conditions associated with inborn errors of metabolism disease, rWGS/urWGS are more likely to return positive results in this patient population. Though, of the four patients who were placed on ECMO for metabolic concerns and had rWGS/urWGS, two had no clinical change based on positive results as changes had already been made based on presumed diagnosis (Table 4). Additionally, assessing clinical utility, especially with negative results, was challenging retrospectively. We found that notes in the electronic health record appeared more likely to note positive rWGS/urWGS results when justifying clinical changes. Further prospective studies into the utility of rWGS/urWGS would better assess the impact of both positive and negative results. We also noted that rWGS and urWGS evolved during our study period as access to urWGS, which provides the fastest time to results, became more readily available.
With increasing access to rWGS/urWGS it is important to understand which patients and clinical scenarios would benefit most. Given the limitations associated with conducting randomized trials on this population, illness severity provides a practical guide, helping clinicians understand when rWGS/urWGS is indicated. Patients who require ECMO are some of the most critically ill patients in the NICU, and this study demonstrates they may be an ideal population for rWGS/urWGS given both the high diagnostic rate and results impacting clinical care. Prospective studies are needed to identify the clinical impact of a universal rWGS/urWGS screening program for neonatal ECMO patients.
{kind=link}
{kind=link}
{kind=link}
{kind=link}