The results of this study suggest that decreases in intraoperative rSO2 below 50% are associated with postoperative delirium after OPCAB. This was also associated with postoperative acute kidney injury and longer ICU and hospital stays. Among patients less than 68 years of age, rSO2 lower than 55% was associated with postoperative delirium. However, in patients more than 68 years old, intraoperative rSO2 was not associated with postoperative delirium.
The incidence of delirium in this study was 12.9%, slightly lower than reported by previous studies using similar diagnostic methods (23% to 52%) [9]. One of the reasons for this difference may be the age of the included patients, half of whom were under 68 years of age. Conversely, previous studies have included mostly patients over 60 years of age [9]. Age is one of the most powerful risk factors for delirium after cardiac surgery [29]. Furthermore, we selected only patients who had underwent OPCAB, while in previous studies both on-pump and off-pump cardiac surgery were included, with on-pump surgery being more common [9, 18, 19, 29]. Although the topic remains controversial, some studies have suggested that beating heart surgery can lower the risk of delirium caused by solid microemboli or the alteration of cerebral autoregulation during the cardiopulmonary bypass (CPB) period[18, 23, 30].
Considering the cut-off values for intraoperative rSO2 during cardiac surgery, Yao and colleagues [17] set multiple thresholds indicating different degrees of hypoxic brain injury. They used 50%, 45%, 40%, 35%, and 30% as absolute values, corresponding to the baseline value minus 1, 1.5, 2, 2.5, and 3 SDs. An rSO2 reduction below 40% was significantly associated with postoperative neurologic dysfunction after cardiac surgery with CPB based on a multivariable analysis. In several studies, including randomized control trials, prolonged cerebral desaturation below 50% as an absolute value or more than 20% of baseline was associated with postoperative cognitive decline [31-34]. However, these studies were mostly conducted on cardiac surgery with CPB and evaluated only one or two thresholds rather than various cut-off ranges.
We aimed to determine whether there is a certain cut-off value for intraoperative rSO2 during OPCAB associated with increased postoperative delirium. Previously, it has been shown that rSO2 values measured by cerebral oximetry reflect a balance between oxygen consumption and supply in the frontal lobe, especially in the “water-shed” area in the junction between the anterior and middle cerebral arteries [3, 16]. Intraoperative cerebral hypoperfusion is also known to be related to postoperative neurological dysfunction after cardiac surgery [17, 30-32]. However, several randomized controlled trials showed inconsistent results regarding the relationship between intraoperative rSO2 reductions during cardiac surgery and postoperative neurologic outcomes. Two meta-analyses focusing on the use of cerebral oximetry and postoperative outcomes after cardiac surgery concluded that there was a low level of evidence linking intraoperative reductions in rSO2 with postoperative neurologic outcomes [13, 35].
There may be several reasons for the inconsistent results regarding the usefulness of cerebral oximetry during cardiac surgery. First, heterogeneous patients were enrolled in previous studies. These studies involved various types of cardiovascular surgeries, including valvar surgery, coronary artery bypass surgery, cardiac tumor surgery, and aortic surgery, which involve different applications of intraoperative CPB and hypothermia. Transient but significant dysfunction in cerebral autoregulation and cerebral desaturation due to hemodilution or microemboli may occur with CPB. Cerebral oxygen consumption is also altered during CPB and hypothermia [14, 15, 17, 18, 36, 37]. Thus, with or without CPB, these heterogeneous populations may have led to inconsistent results. In the current study, to increase the homogeneity of patients, we included only patients who had undergone OPCAB without CPB.
In addition, previous studies including several randomized controlled trials, used various protocols and rSO2 cut-off values to trigger intervention to restore rSO2. This may also have contributed to the inconsistent results. Conversely, we evaluated the relationship between rSO2 reductions and postoperative delirium at various cut-off values. By analyzing not only the occurrence but also the total duration of rSO2 reduction, we aimed to identify the threshold of hypoxia exceeding the compensating capacity of the brain relating to the duration of cerebral desaturation.
We also included intraoperative MAP, C.I., and SvO2 as risk factors for postoperative delirium occurrence. Although these hemodynamic variables can affect intraoperative cerebral perfusion and consequently postoperative delirium, they have not been included in many previous studies. In our study, by conducting a regression analysis, we attempted to rule out the possibility of multicollinearity between these hemodynamic variables and rSO2.
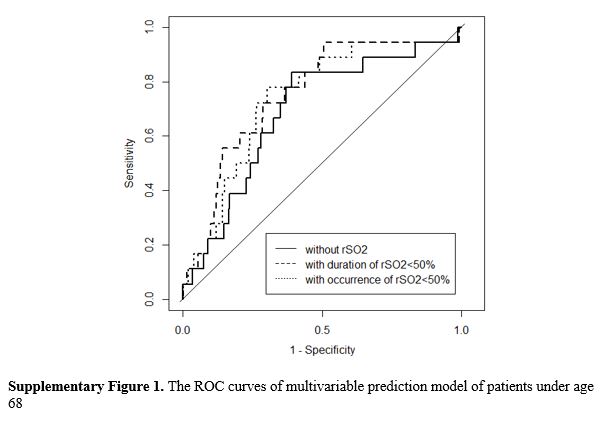
In the subgroup analysis of patients under age 68, only preoperative EF, level of albumin, and C-reactive protein were associated with postoperative delirium by univariable analysis. The cut-off value of rSO2 associated with postoperative delirium was 55%, which was slightly higher than the 50% cut-off for the entire study group. Moreover, in patients over age 68, rSO2 was not associated with postoperative delirium. The pathophysiology of postoperative delirium is complex, and age is one of the most powerful risk factors, along with history of hypertension [6, 9, 19, 21]. Thus, in old patients, other factors associated with old age may more strongly influence the occurrence of postoperative delirium than intraoperative brain oxygenation.
This study has several limitations. First, because this study was retrospective in nature, risk factors that could affect postoperative delirium could not be perfectly controlled. Similarly, the anesthetic management to maintain or restore rSO2 was not controlled. Second, this study involved cardiac surgery cases from 2004 to 2016, and surgical and anesthetic methods and techniques evolved over this period. These changes may have influenced the occurrence of postoperative delirium. Third, preoperative neurologic function was not assessed, and postoperative delirium was estimated using medical records and prescription history. The incidence of postoperative delirium may therefore have been underestimated. Finally, we could not assess the baseline rSO2 values. Previous studies consistently found that preoperative baseline rSO2 was associated with postoperative delirium in cardiac surgery [13, 15, 35]. However, since this was a retrospective study, the impact of baseline rSO2 on postoperative delirium could not be evaluated. Consequently, the decrease in rSO2 relative to the baseline was not estimated. The baseline values for rSO2 vary by its measuring methods according to previous various studies, and most of them require visiting patients before surgery and supplying O2 for several minutes to measure baseline values. In real clinical practice, however, it is not easy to measure and even though it was measured, baseline value itself may not be in normal physiologic values for cardiac surgery patients. The reserves from the baseline values may be different by the individuals. So, based on our experience in clinical practice, we hypothesized that the just ‘cut-off value; may have clinical significance, and that is one of the reasons we started this retrospective analysis without baseline values. We may try to comparative analysis in the prospective study, next time. Considering the limitations of this study, prospective, randomized controlled studies may be needed to evaluate the effect of intervention to maintain rSO2 over 50% (or 55% for patients under 68 years of age) during OPCAB.
{kind=link}