The surgical approach to prostatic hyperplasia has evolved significantly with the use of the robotic platform, and various surgical techniques have been described. Our technique for robotic prostatectomy seems safe and effective for treating BPH.
We observed significant improvements in prostatic symptoms (preoperative vs postoperative IPSS 23 ± 3.6 vs 4 ± 1.6, p < 0.0001), urinary flow rate (6.3 ± 1.3 vs 22.6 ± 3, p < 0.0001), and prostate volume (144 ± 47 vs 26.6 ± 7.2, p < 0.0001). In addition to the improvements described by Patel et al.[10], we believe that our modification allows for safer access to the prostatic apex and surgical planes. Prostate resection occurs under complete visualization when we dissect the specimen in fragments. This approach reduces sphincter traction and facilitates the identification of the boundaries between the capsule and adenoma, allowing for a more anatomical dissection, with better surgical field, improved hemostasis, less bleeding, and better preservation of the bladder neck. Furthermore, even without suturing the prostatic capsule, we found less blood loss than described by other groups [7,11].
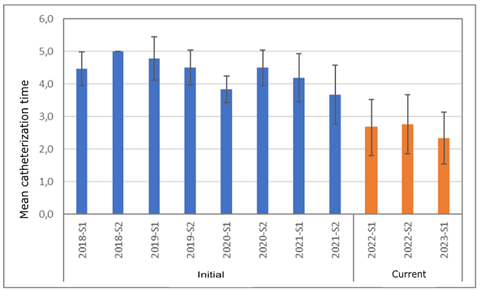
The reduction in catheter time was possible in that we observed good surgical outcomes with very low complication rates. Initially, in selected cases, we began to gradually reduce catheter time while maintaining good results. Today, a good proportion of patients are discharged within 48 hr without an indwelling bladder catheter. Younger patients, with good bladder capacity, good quality of vesicourethral anastomosis, and no postoperative complications are candidates for early catheter removal. Conversely, older patients, on antiplatelet or anticoagulant medications, with previous urinary retention or prior transurethral resection of the prostate, probably have longer catheterization time. In our study, earlier postoperative catheter removal did not affect surgical outcomes or increase the number of complications.
No prospective randomized study has compared RALSP with other techniques. However, a recent review by Kordan et al.[13] demonstrated that the technique can indeed be considered a minimally invasive surgery for prostates > 80 g, showing functional results for IPSS, post-void residual urine, Qmax, and quality of life as well as complication rates, blood loss, and hospitalization time as compared with other techniques such as thulium laser vapoenucleation of the prostate (ThuLEP) and HoLEP.
In a recent meta-analysis[14], RALSP was associated with longer hospital stay and catheterization time and higher TR as compared with laser endoscopic enucleation of the prostate. However, when comparing the results from our study, hospitalization times were similar for RALSP and other techniques (hospital stay 1.6 vs 1.71 days). The same study[14] demonstrated superiority for ThuLEP versus RALSP in terms of surgical time. This superiority was not demonstrated when considering the mean surgical time of our case series (78.7 vs 85 min).
In the meta-analysis of Pandolfo et al.[9], the catheterization time was significantly shorter in patients undergoing HoLEP and ThuLEP than other patients. However, as compared with the second phase of our study, showing decreased catheterization time, catheterization time was shorter for patients undergoing RALSP than those undergoing laser enucleation (2.6 vs 3.54 days). Given these comparisons, RALSP may be superior to other techniques for hospitalization, catheterization, and surgical time.
A potential disadvantage of our technique could be the difficulty in resecting the intravesical component of a larger median lobe. For less experienced surgeons, the lower prostatic exposure due to the subcapsular, extravesical approach might hinder the identification of the intravesical median lobe.
The limitations of this study include its retrospective design and the reliance on results from a single surgeon. However, the number of cases reviewed, the reproducibility of the surgical technique, and the uniformity of the identified data greatly favor the method's applicability.
We believe that access to the robotic platform is increasingly feasible for most urologists, and by providing updated information on the clinical outcomes of robotic adenectomy, we hope to contribute to clinical decision-making and assist colleagues in choosing the best surgical approach for their patients with BHP.
{kind=link}