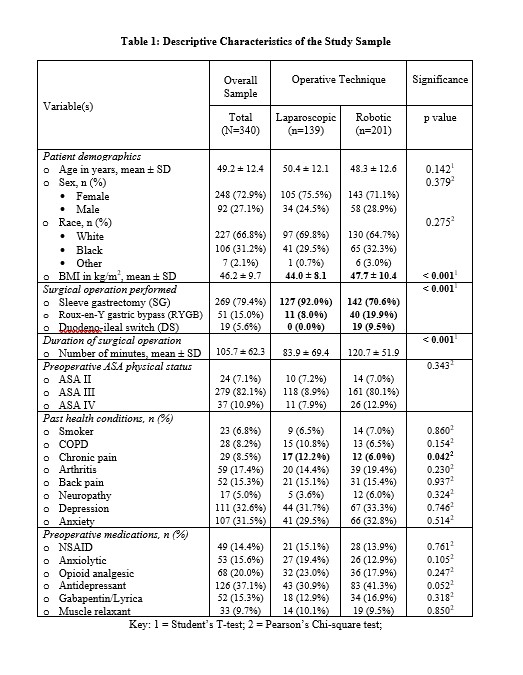
A total of 340 patients received primary bariatric surgery during the study period, of whom 201 (59.12%) underwent robot-assisted procedures while 139 (40.88%) underwent laparoscopy. SG (79.4%) were most frequent, versus RYGB (15.0%) and DS (5.6%) surgeries. SG operations were more likely to be performed via laparoscopy, while more RYGB and all DS operations were robot-assisted. The overall sample was 72.9% female, 27.1% male, 66.8% white, and 37.0% aged 55 years or older; 73.7% had class III (extreme or morbid) obesity (BMI ≥ 40 kg/m2) before surgery. In regards to preoperative mental illness, 32.6% suffered from depression and 31.5% had anxiety. Likewise, 37.1% were taking antidepressants while 15.6% were on anxiolytics before surgery. One of five patients were already taking opioid medications, one of seven were on Gabapentin/Pregabalin, and another one of seven on NSAIDs, before surgery. Median (interquartile range) in-hospital stay after surgery was only 1.0(1.0–1.0) days. Detailed baseline characteristics of the sample are illustrated in Table 1, comparing robotic versus laparoscopic bariatric surgery recipients. The two comparison cohorts did not differ on baseline characteristics (p > 0.05) except for: (a) preoperative BMI, which was significantly higher for robot-assisted versus laparoscopic surgery recipients [mean (± SD) of 47.7 (± 10.4) vs 44.0 (± 8.1) kg/m2, respectively]; and (b) duration of surgery, also higher for robotic procedures [mean (± SD) of 120.7 (± 51.9) vs 83.9 (± 69.4) minutes; p < 0.001)].
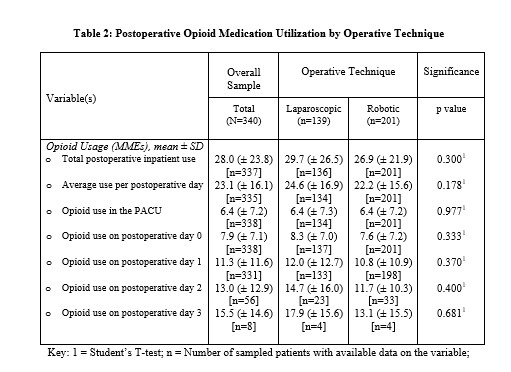
Total in-hospital, pre-discharge opioid utilization after surgery for the overall sample reached a mean (± SD) of 28.0 (± 23.8) MMEs. Daily opioid analgesia administration in the postoperative, pre-discharge period averaged 23.1 (± 16.1) MMEs per day. Mean (± SD) usage increased from 6.4 (± 7.2) in the PACU to 11.3 (± 11.6) on the first day then, for those still admitted, to 15.5 (± 14.6) MMEs by the third day after surgery. As shown in Table 2, postoperative in-hospital opioid consumption did not significantly differ among recipients of robotic versus laparoscopic bariatric surgery. In the multivariable risk-adjusted model of average daily opioid utilization, male sex (β=-4.43; [95% CI: -8.49, -0.36]; p = 0.034), older age (β=-6.77; [CI: -11.76, -1.78]; p = 0.041), depression (β=-6.24; [CI: -11.03, -1.46]; p = 0.011), and being on NSAIDs before surgery (β=-6.11; [CI: -11.29, -0.94]; p = 0.021) were protective factors. Conversely, back pain (β = 4.87; [CI: -0.18, 9.91]; p = 0.058) and being on opioids (β = 8.04; [CI: 3.13, 12.95]; p = 0.001), or Gabapentin (β = 7.44; [CI: 2.15, 12.73]; p = 0.006) at baseline were exacerbators. Figure 1 illustrates these findings. In the multivariable model of the total postoperative, predischarge opioid consumption, being depressed (β=-10.17; [CI: -17.11, -3.22]; p = 0.004) and on NSAIDs at baseline (β=-7.75; [CI: -15.29, -0.22]; p = 0.044) were protective while having back pain (β = 9.47; [CI: 2.14, 16.780]; p = 0.012) and being on opioids before surgery (β = 14.74; [95% CI: 7.61, 21.86]; p < 0.001) exacerbated the risk of greater usage. This model is depicted by Fig. 2.
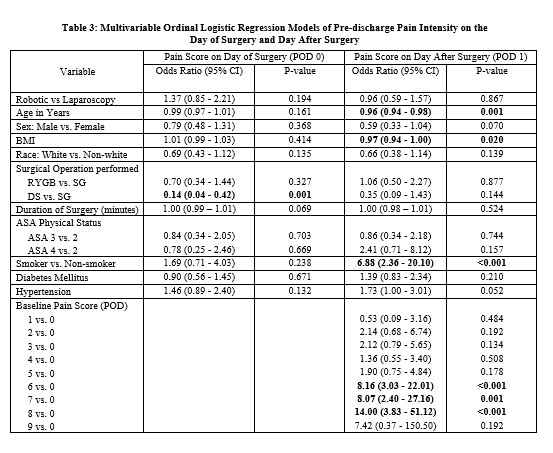
In multivariable ordinal logistic regression models of POD0 and POD1 VASP scores, perceived pain intensity was NOT significantly higher for patients undergoing robotic versus laparoscopic primary bariatric surgeries, after accounting for other risk factors. In these models, male sex (OR = 0.59; [CI: 0.33, 1.04]; p = 0.07), higher BMI (OR = 0.97; [CI: 0.94,1.00]) and older age (OR = 0.96; [CI: 0.94, 0.98]; p = 0.001) were associated with reduced odds of greater pain intensity on POD1, and being a smoker at the baseline with increased odds (OR = 6.88; [CI: 2.36, 20.10]; p < 0.001) of higher pain intensity on POD1, independent of other risk factors. DS (versus SG) operations were associated with lower odds (OR = 0.14; [CI: 0.04, 0.42]; p = 0.001) of higher pain ratings on POD0, independent of covarying factors. Odds ratios from the multivariable ordinal logistic regression models are summarized in Table 3.
{kind=link}
{kind=link}
{kind=link}