This study revealed that patients undergoing metabolic surgery in the Netherlands from 2015 to 2023 were, irrespective of their BMI level, increasingly assigned an ASA-PS III score. Furthermore, it showed that in this selected populations, patients with a BMI ≥ 40 kg/m² without severe systemic disease, showed a significantly lower likelihood of experiencing surgical complications during their metabolic surgery -trajectory compared to patients with a BMI < 40 kg/m² and severe systemic disease. Additionally, they exhibited reduced probabilities of prolonged hospital stay, readmission, planned, and unplanned ICU admission. These results confirmed our hypothesis.
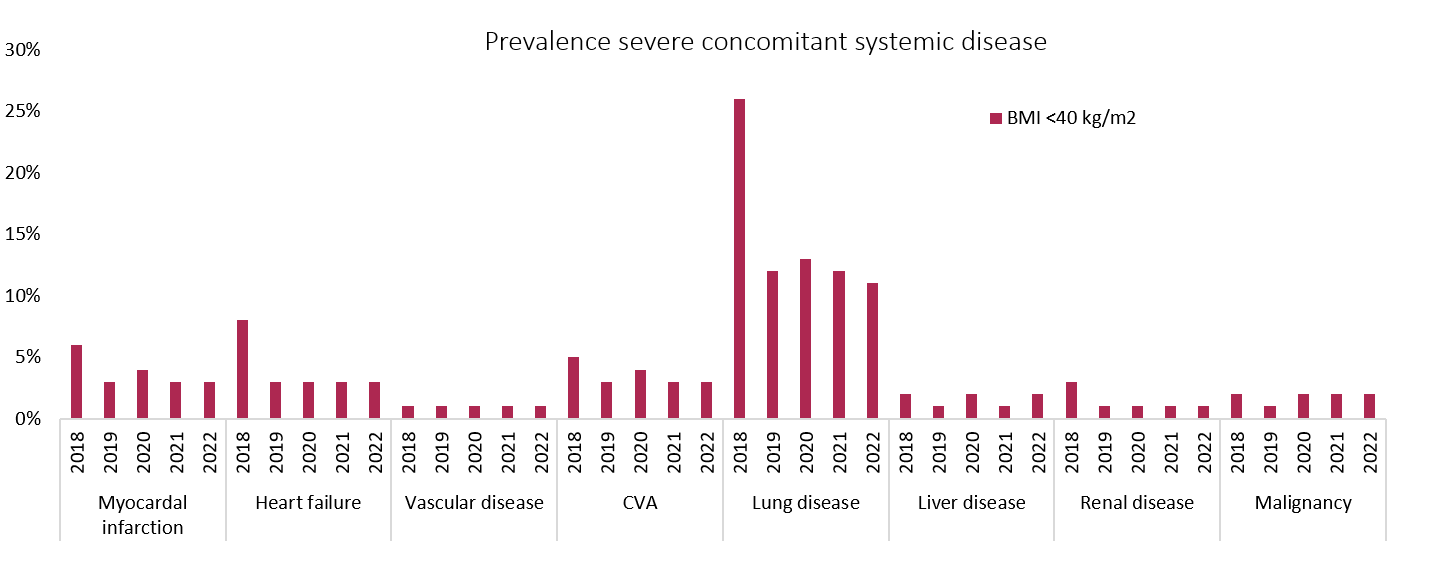
ASA-PS classification is a simple and fast way to gain insight into the patient's health status and estimate postoperative risk26. The increase in ASA-PS III scores can largely be attributed to changes in the guidelines: Without taking into consideration co-morbidity or physical status, patients with a BMI ≥ 40 kg/m² switched from score II to III. Notably, also patients with a BMI < 40 kg/m² increasingly received an ASA-PS III. We have objectified that between 2018–2023, patients were incorrectly assigned an ASA-PS III score in 60–70% of cases. These patients had a BMI below 40 kg/m² and no severe concomitant systemic diseases. Even before 2018, the population did not suffer from concomitant diseases more frequently, which may suggest that the unjustified allocation had started earlier. Although the ASA-PS classification guidelines have been made as objective as possible, it is well known that it remains subject to interpretation27–29. We hypothesize that by raising awareness about criteria for determining an ASA-PS classification through the introduction of a new guideline, stricter assessments and subjective up-coding leading to higher scores has occurred. Although the context differs, this effect bears some resemblance to the Hawthorne effect in terms of behavioural changes in response to external factors30.
The presence of a serious systemic disease appeared to have a greater impact on the occurrence of complications during a metabolic surgery procedure compared to a BMI > 40 kg/m². Although both are categorized as ASA-PS III, the operative risk profiles as assessed by the ASA-PS classification were not identical. Considering the observation that the rate of complications among patients with a BMI > 40 kg/m² closely mirrored that of patients with a lower BMI, it indicates insufficient evidence to support the BMI-criterion in our study population. Using BMI > 40 kg/m² as sole criterion for ASA-PS III classification undermines the efficacy of risk stratification in clinical practice. Accurate ASA-PS classification at the individual level, would guarantee more precise allocation of hospital resources, better decisions regarding inpatient or outpatient surgery and timing of hospital discharge, and facilitating the delivery of personalized care efficiently while maintaining safety standards. Moreover, incorrect ASA-PS classification can result in research outcomes or quality evaluations that present a skewed perspective, rendering them unsuitable for reliable interpretation and implementation in clinical settings. Previous research in patients undergoing metabolic surgery showed a minimal difference in complications between ASA-PS II and ASA-PS III patients31. This could be explained by the fact that the results were based on the assigned ASA-PS classification and not on the actual underlying disease thereby reflect clinical practice inaccurately.
BMI has frequently faced criticism as a metric of obesity severity or the risk of comorbidities or complications32–34. Instead, it is rather a static representation of a patient's body composition at a given point in time, while for example, long-term exposure to excess adipose tissue appears to be crucial in the development of obesity-related complications35–38. Therefore, the inquiry arises regarding the suitability of the BMI metric for assessing health status altogether. Functional status or cardiorespiratory fitness, for instance a Metabolic Equivalent Score, is also widely used in preoperative screenings. It is a measure the amount of oxygen the body consumes during an activity compared to a resting state39 and can be used to estimate whether the patient is able to withstand the physical demands of surgery regardless of age, body composition, or comorbidities40. Functional status is correlated logically with the ASA-PS classification, as illness could lead to immobility and vice versa, however functional status has also been shown to be a better predictor than the ASA-PS classification itself31. It would be interesting to further explore the effect of incorporating functional status to the ASA-PS classification, instead of or in addition to BMI, as there are already indications that the latter is an independent predictor of mortality within each ASA-PS classification41.
The recategorization of patients for concurrent systemic diseases was dependent on a diagnosis code, which was not always distinctive in terms of severity of the condition. This could be seen as a limitation of the study. For instance, hypertension encompassed both treated stable hypertension and untreated unstable hypertension, posing a potential risk of underestimating research results. Nonetheless, this method still remains closely aligned with the current clinical practice, where the ASA-PS classification is not entirely comprehensive. In addition, information regarding smoking status or alcohol use was absent. Although these factors may not directly differentiate between ASA-PS classifications, they should be taken into account as they may increase the risk of postoperative complications independently42,43. Due to the limited number of cases with multiple complication registrations, a multilevel analysis was not performed. This could lead to repeated-measure bias, affecting the accuracy of effect size estimation. Notably, both the highest complication prevalence and majority of patients who experienced more than one complication were identified in the subgroup characterized by BMI < 40 kg/m² and severe systemic disease. Given the direct link between repeated measurements and complications in this context, the exclusion from multilevel analysis can be considered less problematic.
This study was strengthened by the large size of the cohort. The results are representative of Dutch clinical practice and may also be applicable to other countries with similar patient populations levels of surgical selection or preparation and, importantly, a comparable healthcare system. The homogeneity of the cohort reduces the risk of bias in this setting. We suggest that future research should investigate the relationship between increasing BMI and peri-operative complications to determine whether different BMI thresholds may offer greater accuracy. Additionally, although beyond the scope of this study, exploring other metrics that might serve as better indicators of health status and risks for patients living with obesity would be valuable to consider. Also, our hypothesises could be examined in other cohorts undergoing metabolic surgery or in patients undergoing other surgery types.
We conclude that due to changed guidelines, patients undergoing metabolic surgery in the Netherlands were increasingly assigned ASA-PS III, irrespective of BMI or concomitant systemic disease suggesting subjective upcoding. However, patients from this ASA-PS class based on solely a BMI ≥ 40 kg/m² were less likely to have a complicated course after metabolic surgery than patients with a severe systemic disease. This finding suggests a devaluation of the value of ASA-PS in peri-operative risk stratification in patients living with obesity by sticking to a sole rigid criterium. It has significant implications for enhancing peri-operative resource utilization and improving efficiency without compromising safety. Correcting the overestimation of ASA-PS classification in patient assessments can not only contribute to more accurate risk stratification but also improve the overall validity of research results incorporating ASA-PS classification.
{kind=link}