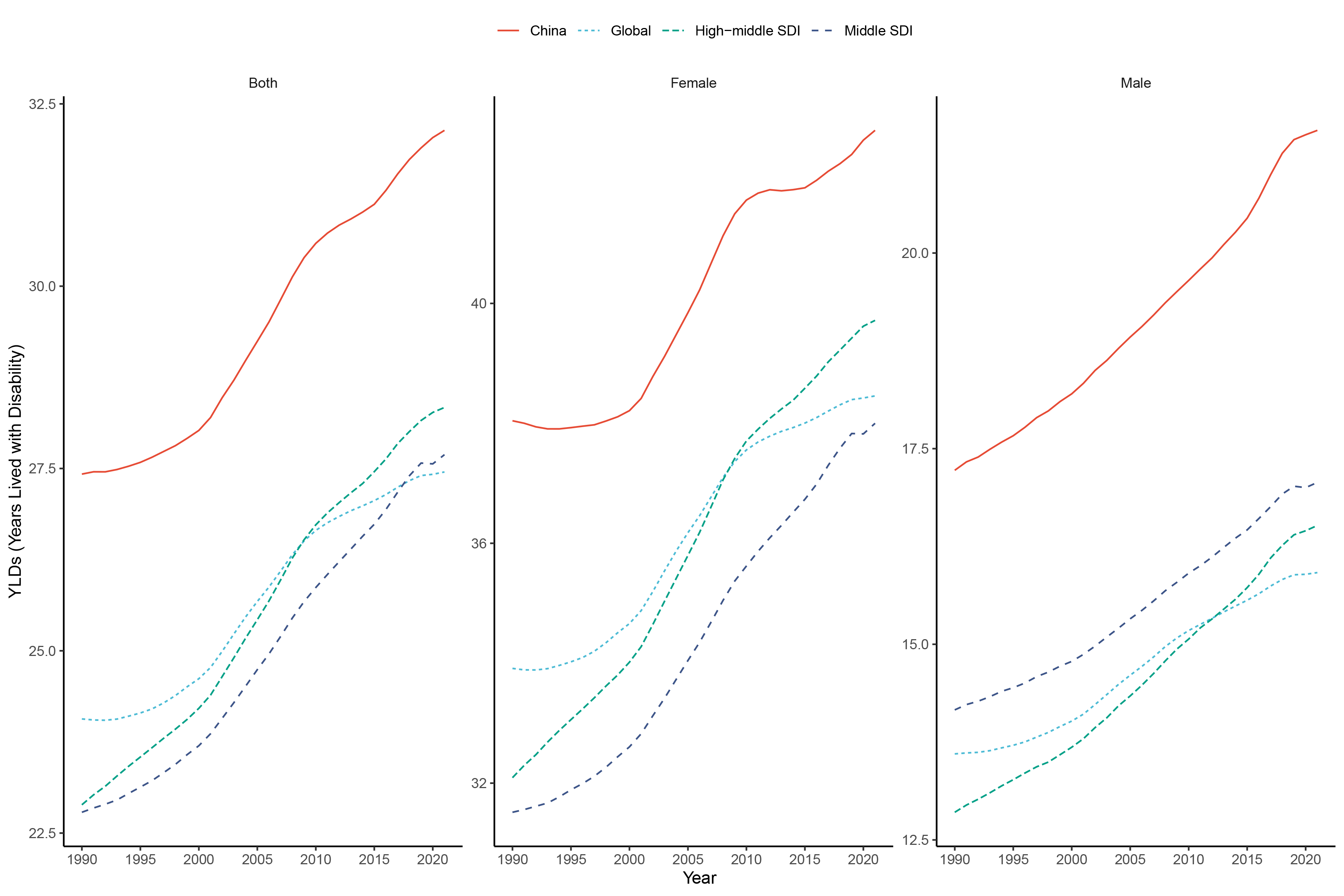
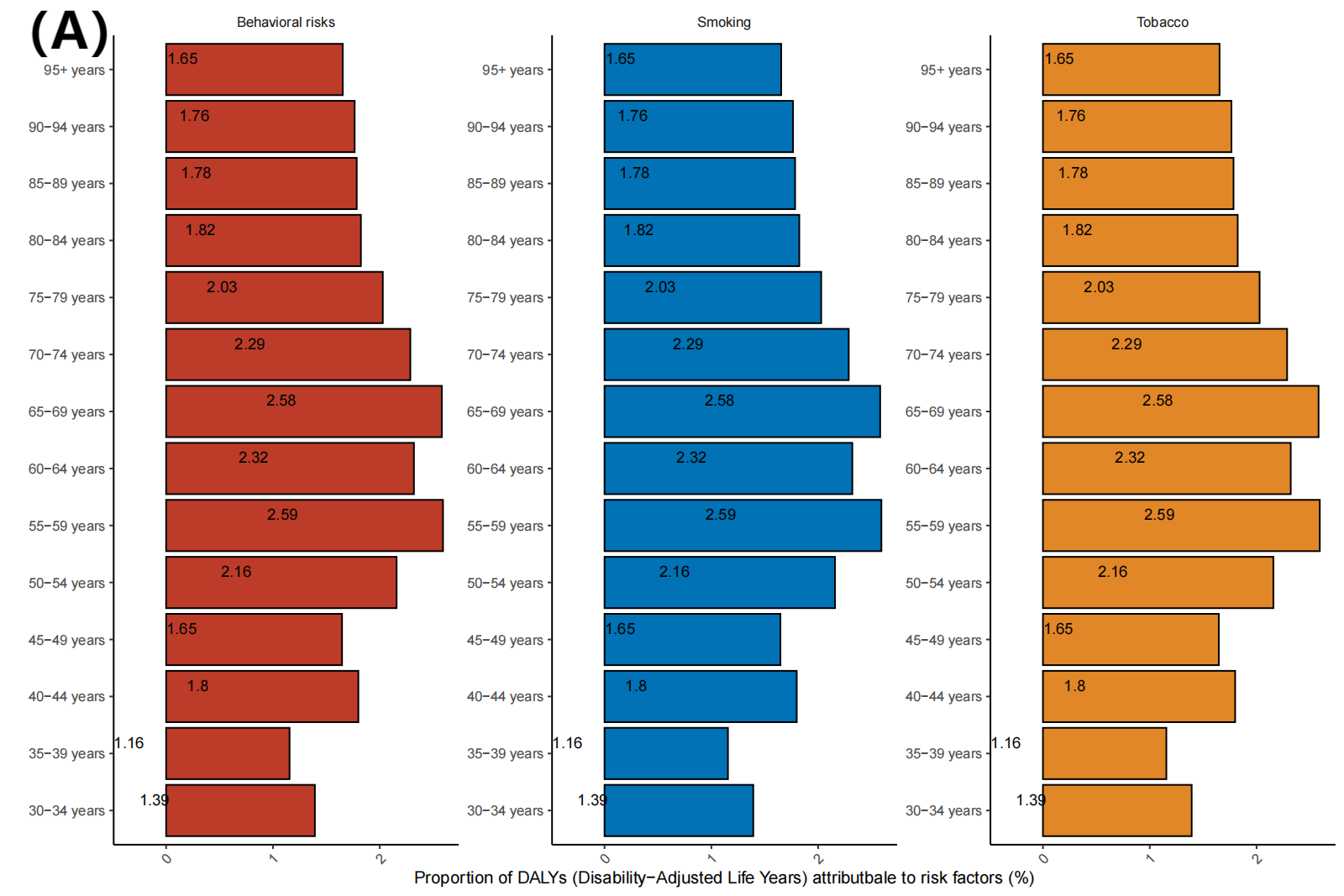
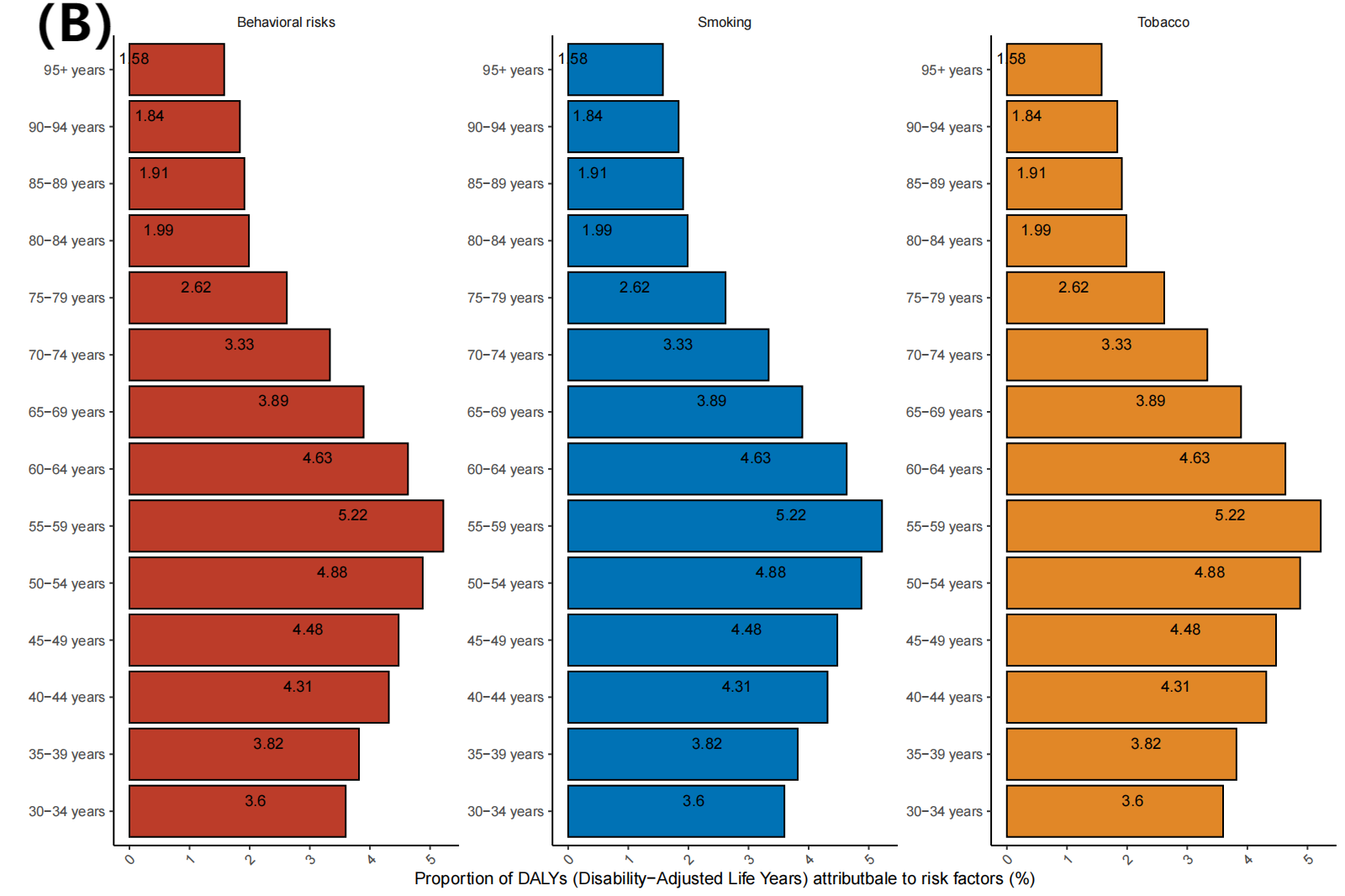
RA represents a significant global public health concern, with a considerable body of research dedicated to understanding its impact on prevalence and mortality. The present study encompasses a 30-year period and provides a comprehensive description of the disease burden in diverse populations over time. In 2021, the age-standardized prevalence of RA in China was estimated at 240.695 cases per 100,000 people, notably exceeding the global average. These findings suggest that China is a high-risk area for RA (Fig. 6)[23, 24]. As of 2021, the estimated number of RA patients in China is 4,755,487, nearly doubling over the past three decades. Concurrently, the age-standardized prevalence has also dramatically increased. This is significantly higher than the global average, as well as the averages for high-middle and middle SDI countries. The burden of RA due to disability constitutes more than 60% of total DALYs, surpassing both the global average and the averages of High-middle and Middle SDI countries with similar economic development to China (Fig. 5). Furthermore, our findings indicate that adults continue to represent the most affected demographic, with the highest DALY rates observed among individuals aged 55–59 years in China. These findings highlight the significant burden of RA in China, underscoring the need for improved management strategies.
Prior research has revealed notable regional differences in the prevalence of RA in China[7–9]. These discrepancies may be attributed to various factors, including different time periods, statistical methodologies, and economic levels. Additionally, the occurrence of RA may be influenced by genetic, climatic, and environmental factors[25, 26]. In July 2020, the National Clinical Medical Research Centre for Skin and Immunological Diseases published the China Rheumatoid Arthritis Development Report 2020, which indicated that RA is among the top 10 chronic disease prevalence rates among Chinese residents, with a prevalence rate of approximately 0.42% in mainland China. Despite a prevalence of 5 million people, China’'s large population base makes this disease a significant public health burden. This study presents a comprehensive analysis of RA prevalence, revealing a crude rate of 240.695 per 100,000 people in 2021, which is consistent with previous findings. The increase in the national prevalence of RA may be attributed, at least in part, to improvements in diagnosis and management[27]. Advancements in diagnostic techniques and criteria for RA, coupled with their widespread clinical use, have decreased misdiagnosis and underdiagnosis, indirectly leading to a higher observed prevalence of RA [28].
The GBD 2021 study estimates that RA prevalence is significantly lower in men than in women, irrespective of geographical region, socioeconomic status, or sex. In all regions, the prevalence of females is nearly double that of males. Studies from China and the United States indicate a significantly higher prevalence of RA in females compared to males. These findings align with those reported in this study[29, 30]. Prior research has demonstrated that RA can manifest at any age, with the female population exhibiting a high prevalence of the disease. Numerous observations have postulated that alterations in sex hormone levels may influence the pathogenesis of RA[31]. However, women are more prone to induce modifications in hormone and metabolic levels due to physical disparities (including genetic variations). Additionally, physiological factors, such as menstruation, pregnancy, childbirth, and breastfeeding, as well as lifestyle and occupational influences, can potentially impact the immune system. The more severe and complex condition of female patients could explain the higher disease prevalence in females compared to males[32–34]. It is therefore recommended that clinicians consider sex as a factor in the individualized treatment of RA.
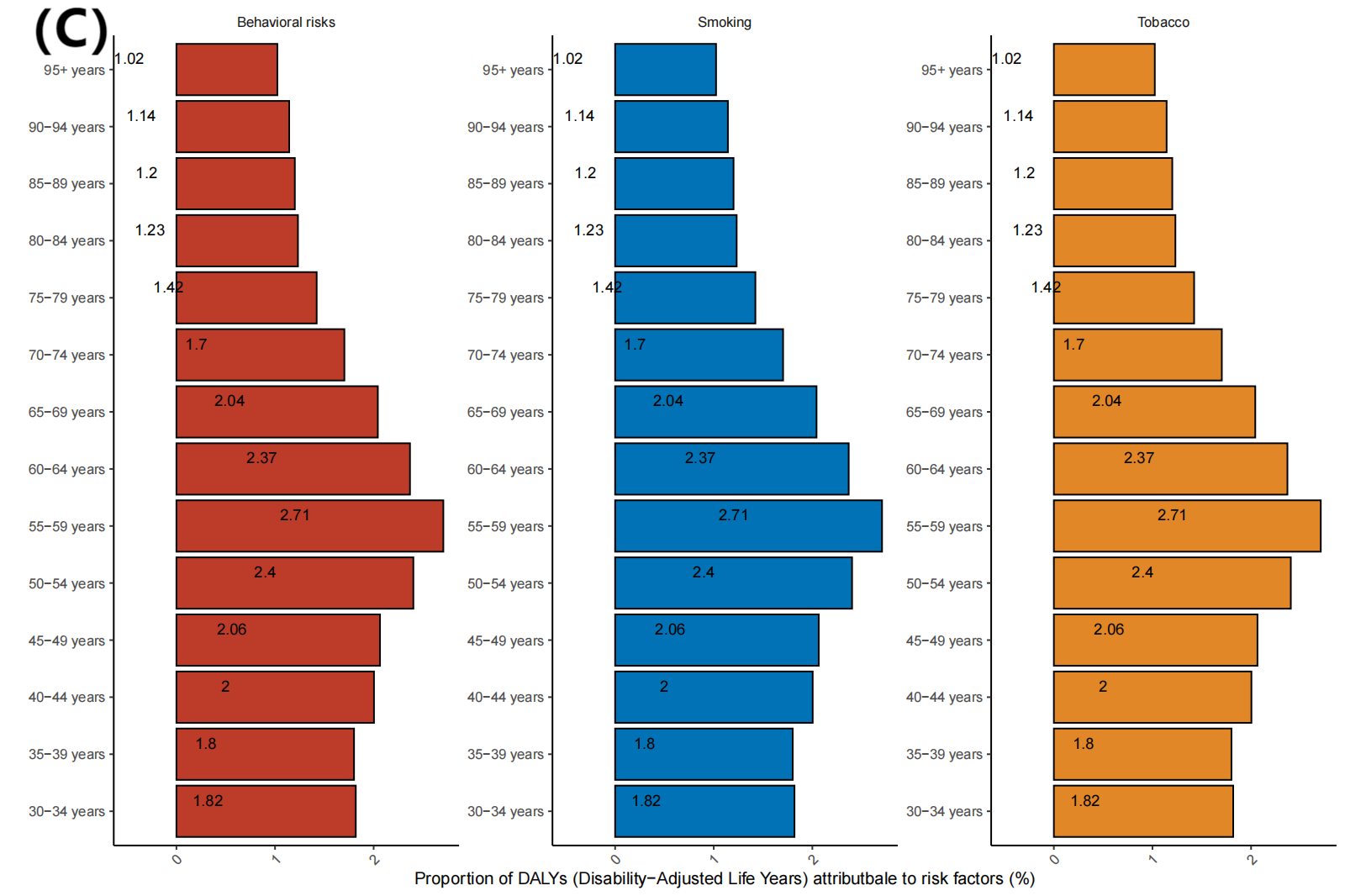
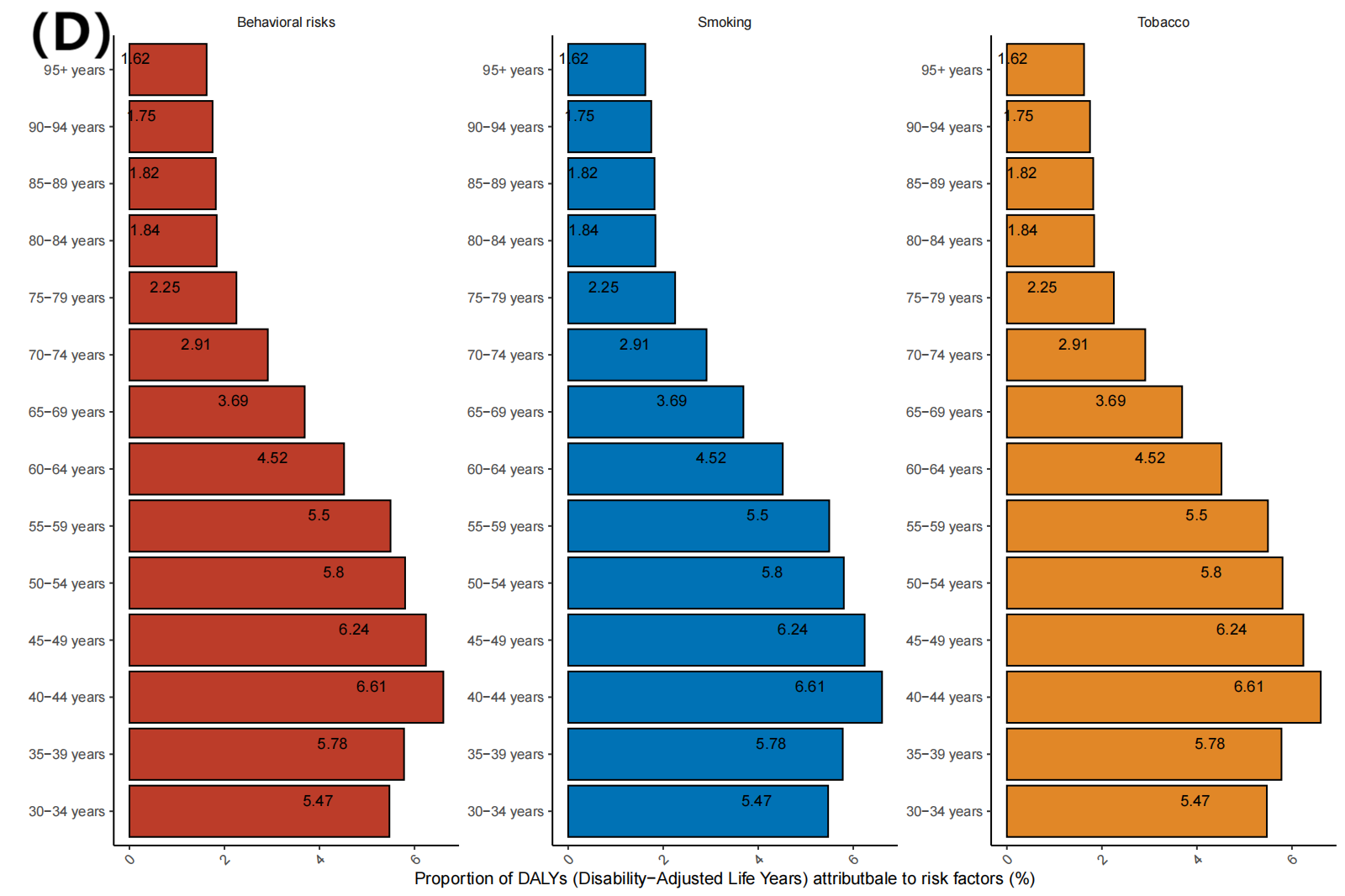
The GBD data indicate a strong association between RA development and risk factors such as smoking and behavioral patterns (Figure S3). This finding has been corroborated by previous studies[35, 36]. Evidence suggests that lifestyle interventions, such as smoking cessation, maintaining a healthy weight, and adhering to a healthy diet, can reduce disease activity in RA patients[37]. Screening first-degree relatives of early-stage RA patients can help identify their risk and enable targeted prevention strategies to reduce disease prevalence.
RA is linked to a higher mortality risk. Compared with the general population, patients with RA may have a reduction in expected survival of between three and ten years. The primary causes of death in this group are malignant tumors, respiratory diseases, and cardiovascular diseases[38]. This suggests that there is a need for greater emphasis on the management of comorbid RA diseases. Furthermore, RA disease activity is also strongly associated with mortality[39]. Survival rates are expected to rise due to advancements in treatment paradigms over recent decades, including early intervention[40] and modernized therapies[41]. Data from the GBD show that age-standardized mortality rates in China, globally, and in countries with high-middle and middle SDI peaked around 2005 for the period 1990 to 2021, and have declined over time since then. Since the 21st century, the strengthening of China’'s rheumatology disciplines, the deepening of RA precision medicine, and the advent of individualized treatment have effectively slowed and stopped the progression of RA in patients in China. Currently, in addition to traditional therapeutic drugs, the popularization and application of novel RA therapeutic drugs such as targeted drugs for specific inflammatory mechanisms in China[42] have markedly enhanced the clinical treatment compliance rate of patients and prolonged their survival, which may be a contributing factor to the reduction of in RA mortality. Notwithstanding the aforementioned advances in treatment and early diagnosis, challenges persist. These include drug availability, financial constraints, insufficient specialists, and specialized care, which remain present in some areas[43]. On the basis of these data, future prevention and control strategies for RA should be assessed and enhanced in accordance with population dynamics and healthcare practices.
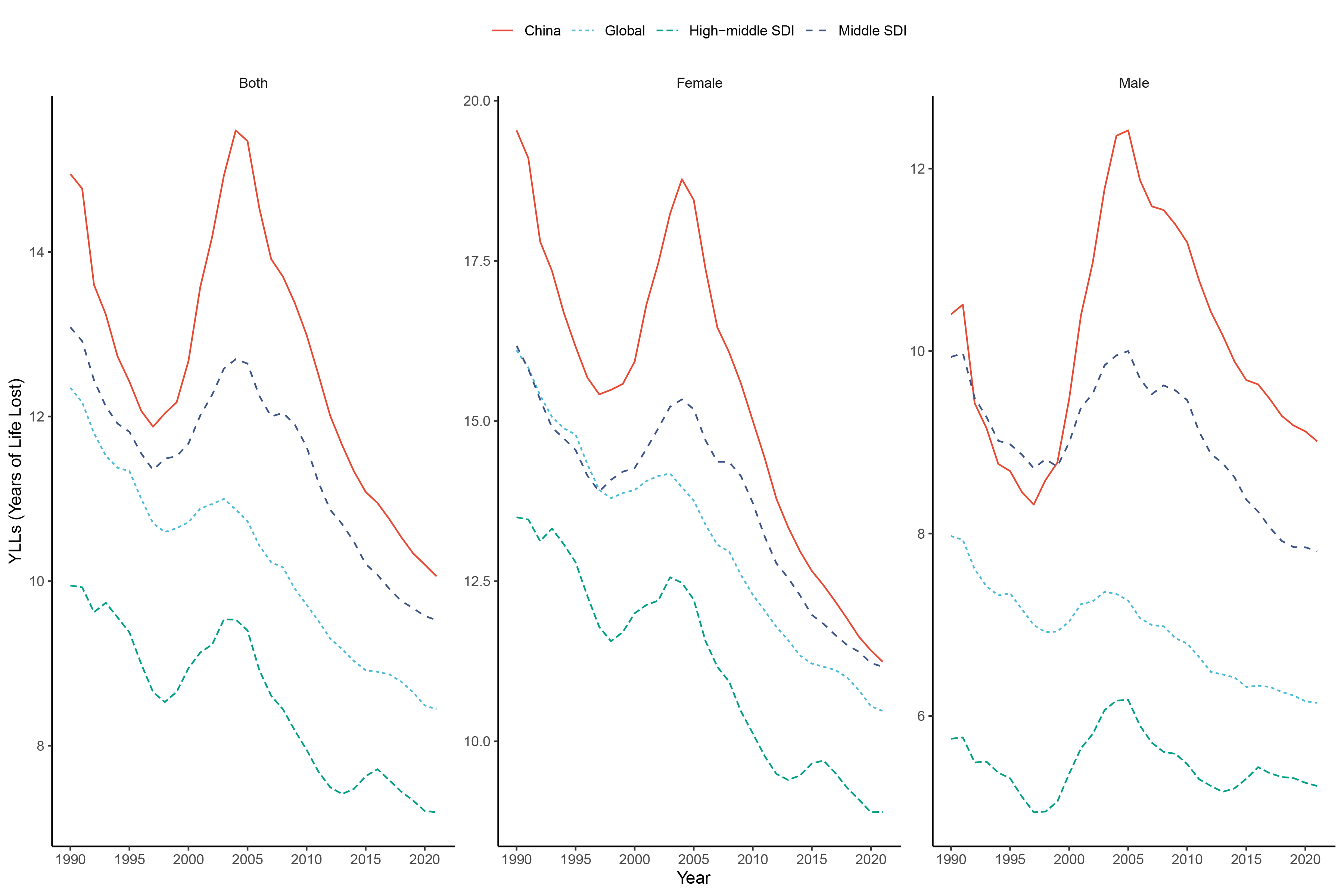
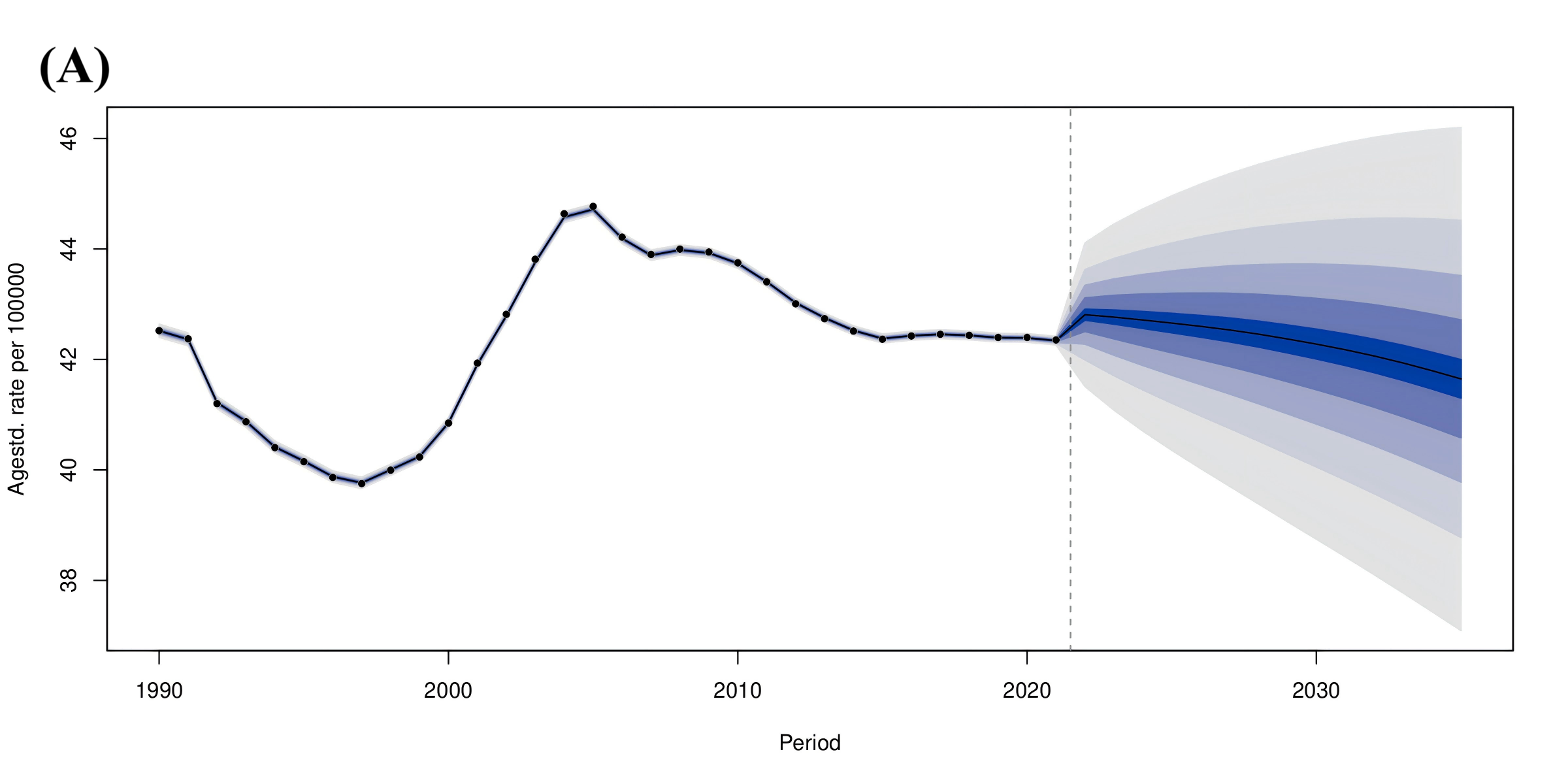
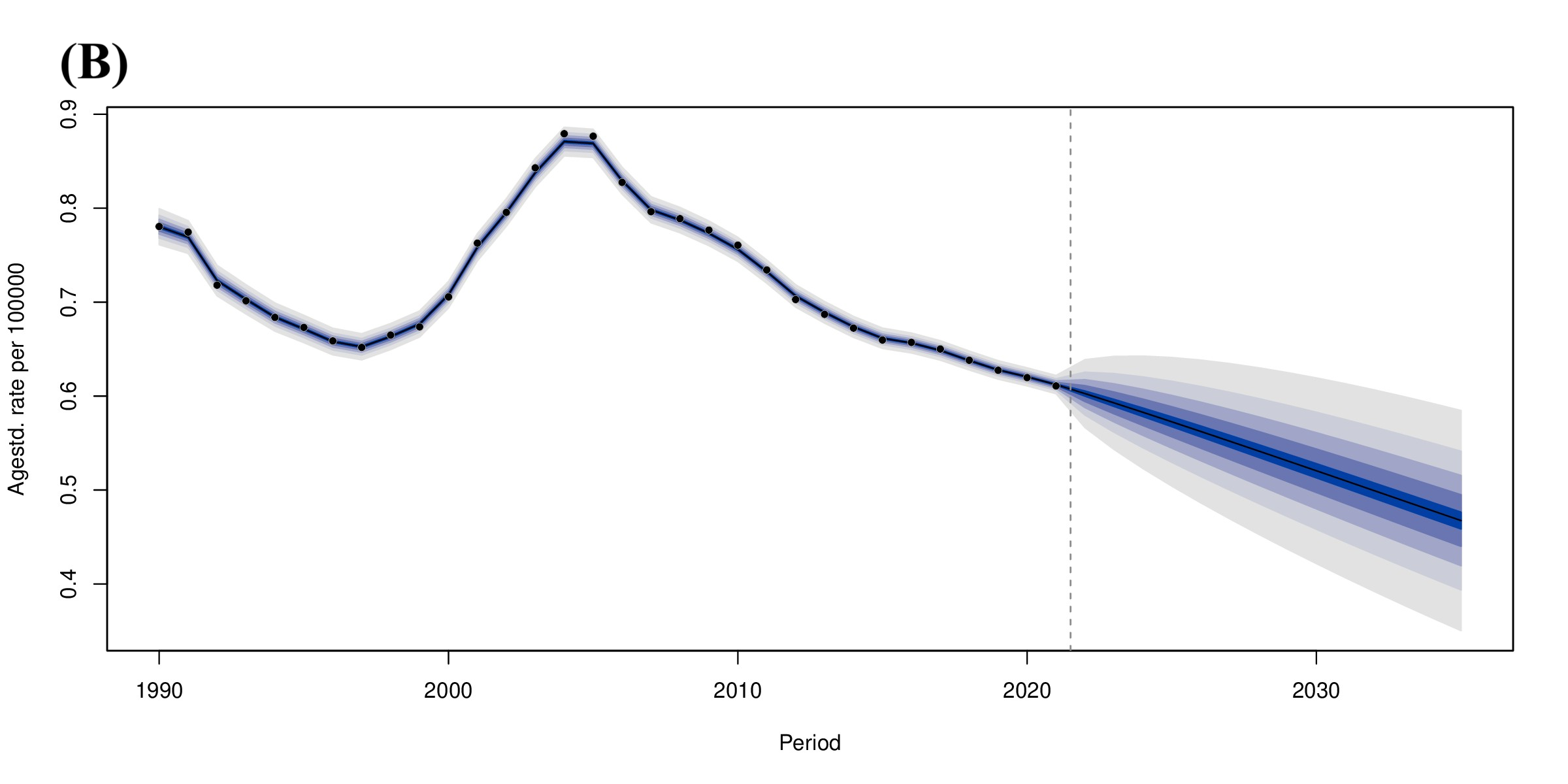
This study revealed that age-standardized DALY rates in China, globally, and in high-middle and middle SDI countries exhibited consistent trends. Age-standardized YLL rates showed similar variations to DALY rates, whereas age-standardized YLD rates experienced significant increases. The DALY in China mainly consists of disability, likely due to insufficient management of RA.RA is a highly disabling autoimmune disease, with joint destruction largely irreversible once it occurs. Previous studies indicate that if left untreated, the 3-year disability rate can reach up to 70% [44]. In China, the average time from symptom onset to definitive diagnosis for patients exceeds two years, indicating a missed opportunity for RA treatment. The median disease duration of Chinese RA patients is 3.86 years, and the cross-sectional disease remission rate is only 4.27%, which is significantly lower than the remission rate of approximately 20% reported in developed countries. Furthermore, among patients not treated with bDMARDs or csDMARDs, 38.84% and 38.11% of patients, respectively, had moderate and high disease activity. Additionally, approximately 4.2% of patients had comorbidities[45]. Additionally, studies from the National Rheumatic Disease Data Center (CRDC) have demonstrated that the issue of unregulated medication use for RA in China is a significant concern. The utilization of methotrexate, hydroxychloroquine, and other primary medications for RA initial treatment is considerably lower than the global standard in China. Furthermore, patients exhibit inadequate awareness of the necessity for standardized RA treatment, and Chinese RA patients demonstrate lower treatment adherence and a lack of long-term regular follow-up. Currently, there is a dearth of guiding standards for the management of chronic rheumatic diseases and standardized chronic management models with evidence-based medical evidence [46]. These factors contribute to the increased disability rate and higher DALYs in Chinese RA patients. Fortunately, since 2017, several new medications have been approved and introduced into clinical practice, including JAKi inhibitors such as tofacitinib and baricitinib, and biologics such as adalimumab and infliximab. These developments are anticipated to contribute to slowing the progression of severe disability in RA patients[47].To further assess the risk of DALYs and mortality risk of RA in China in the future (2035), we employed the method of Riebler A and Held L[48], which is based on the available continuous data, and utilized the Bayesian Age-Period-Cohort(BAPC) model. This model offers a comprehensive framework for projections using integrated nested Laplace approximations (INLAs) for Bayesian inference and data prediction. The findings indicated a decline in the risk of DALYs and mortality (Figures S4).It is anticipated that the advancement of RA disease management in the future will prove instrumental in reducing the disease burden.
The present study has several notable strengths, and monitoring trends in the burden of RA is crucial for the development of public health policies. Our study provides the latest estimates of RA prevalence and mortality in the Chinese population. The primary strength of this study is its extensive coverage spanning nearly three decades, surpassing the scope of most prior research. Furthermore, this study offers valuable insights into RA mortality, a topic that is currently underrepresented in the existing literature. This study has several limitations, including the reliance on global GBD RA data from a limited number of countries, potentially resulting in data incompleteness and affecting the accuracy of burden estimates and the certainty of observed trends. Second, discrepancies in the diagnosis, documentation, and reporting of the disease in disparate countries and regions may impinge upon the comparability of the data. Future research should prioritize incorporating more high-quality studies to increase estimation accuracy. Third, China’'s extensive geography and significant socioeconomic disparities, coupled with insufficient provincial data analysis, may have led to healthcare inequalities and an underestimation of the disease burden in less developed regions. Our study highlights the necessity of addressing the RA burden in diverse populations, especially in densely populated Asian countries.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}