Identification of angiogenesis-associated gens with prognostic significance in LAML
The flow chart of this work was shown in Fig. 1A. A total of 233 genes were found to be significantly associated with prognosis of LAML (P < 0.05) from GSE37642 dataset, and 1137 angiogenesis-associated genes were obtained from the GeneCards database, containing 8 genes significantly associated with prognosis of LAML. Thus, we selected these 8 genes as candidate targets, which were further screened using LASSO analysis and verified using TCGA_LAML dataset. We ultimately identified 5 angiogenesis-related genes that associated with prognosis (Figures S1 and S2), namely ECM1, EGLN1, FKBP5, FOXP1, and SIRT2. Further Kaplan-Meier curves delineated that high expression of ECM1, EGLN1, FKBP5, and SIRT2, whereas low expression of FOXP1 were related to worse prognosis (Fig. 1B and 1C).
Cluster classification was implicated with the malignancy of LAML
To investigate the overall prognostic value of these 5 genes, we conducted a consensus clustering analysis to classify LAML patients, showing that k = 2 appeared to be a more stable value than that of k = 3–6 (Figs. 2A and 2B). PCA was further employed to validate the reliability of the cluster, indicating that, when k = 3–5, the samples showed high similarity and clustered together (Figure S3). Thus, we stratified the LAML patients into 2 clusters. The Kaplan-Meier curves demonstrated that patients in cluster 1 had a poor prognosis than those in cluster 2 (Fig. 2C).
Construction and validation of an angiogenesis-associated prognostic signature
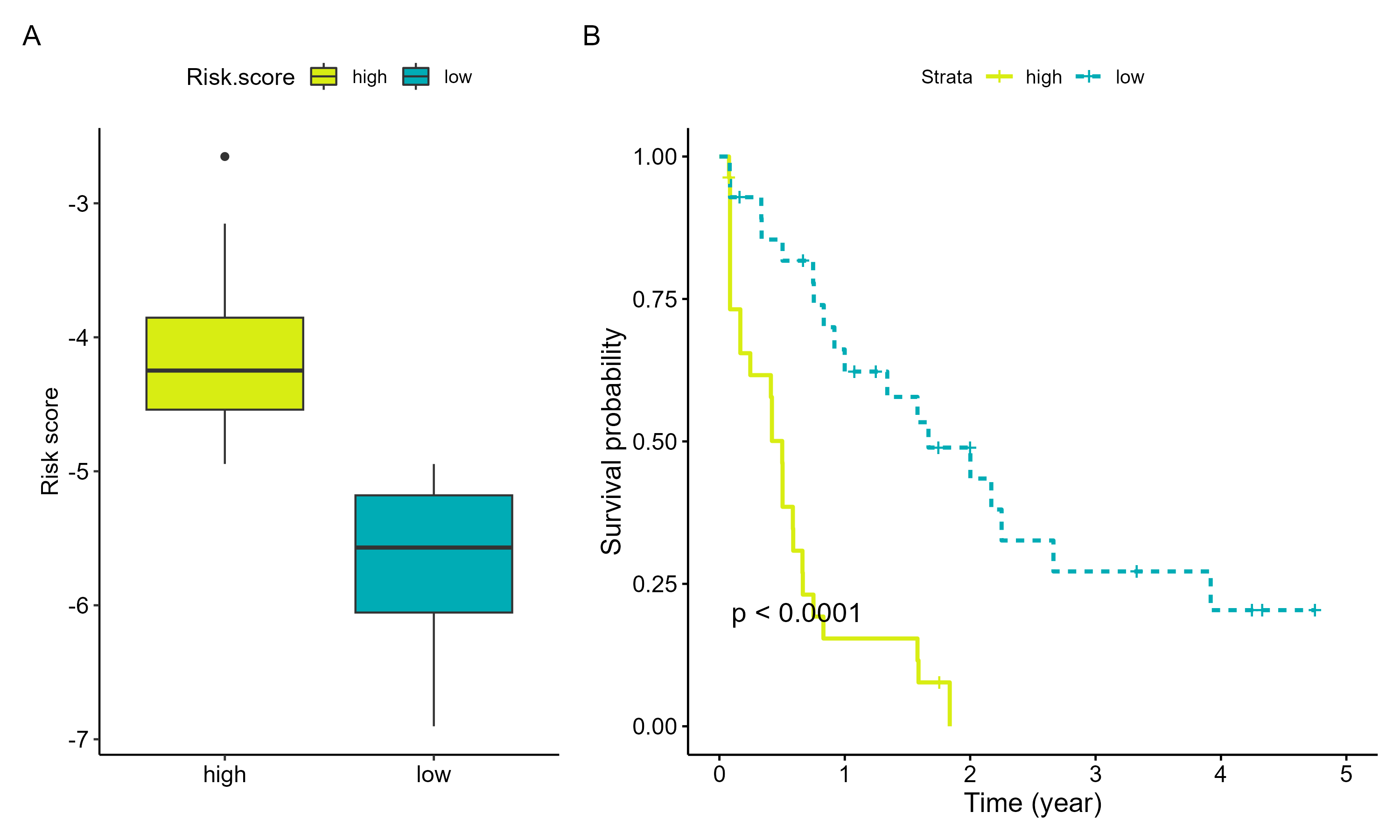
Risk scores for prognostic signature of LAML patients were constructed based on the coefficients and expression levels of 5 selected genes. The detailed formula was shown below: Risk score = 0.5285351*ECM1 + 0.2861940*EGLN1 + 0.3392907*FKBP5-0.5082985*FOXP1 + 1.0852212*SIRT2. The patients were classified into low- and high-risk groups based on the median risk score, and Kaplan-Meier curves showed that patients with high-risk had worse prognosis compared with those with low-risk (Fig. 2D). The prognostic characteristics were then validated in TCGA_LAML dataset, showing the similar result of GSE37642 dataset (Figure S4). These results demonstrate the reliability and stability of the prognostic characteristics. Further analysis identified risk score as an independent risk factor for prognosis of LAML patients (Figs. 2E and 2F).
Identification of the prognostic signature-related biological pathways
We selected genes closely related to the risk score to explore potential biological pathways associated with prognostic signature, including 915 positively correlated genes and 187 negatively correlated genes. The enrichment analysis results of GO and KEGG pathways are shown in Figs. 3A, 3C, and 3E. The GO analysis primarily enriched in actin filament organization, while the KEGG analysis primarily enriched in salmonella infection. The results of GSEA analysis show that high-risk samples are mainly enriched in immune-related pathways (Figs. 3B, 3D, and 3F).
The associates with the tumor immune microenvironment and drug sensitivity
As depicted in Fig. 4A, remarkable disparities in the infiltration of immune cells can be observed between high- and low-risk patients, with intricate variations in the proportions of various immune cells. Subsequent analysis unveiled that, in comparison to high-risk patients, low-risk patients exhibited reduced immune scores and heightened tumor purity (Fig. 4B). Correlation analysis demonstrated a robust association between 5 selected angiogenesis-associated genes with and immune cells, potentially implicated in the regulation of patient prognosis (Figs. 4C and 4D). Evaluation of drug sensitivity in LAML patients using 198 drugs revealed significant discrepancies in IC50 values between high- and low-risk groups for 6 drugs, namely AZD7762, BI.2536, Daporinad, AZD5582, ULK1_4989, and ABT737 (Fig. 5A). Notably, the gene FOXP1 displayed a negative correlation with Daporinad, ABT737, and BI.2536, while SIRT2 exhibited a positive correlation with ABT737, BI.2536, and ULK1_4989 (Fig. 5B and Figure S5).
{kind=link}