Eligibility criteria {10}
Inclusion criteria
Patients who meet the following conditions will be included:
(1) 18–70 years old, male or female;
(2) Patients who will undergo gastroscopy with local anesthesia;
(3) Clear consciousness, can answer the questions, understand the scales and complete the assessment;
(4) Agree to participate and sign a written informed consent.
Exclusion criteria
Patients who meet any of the following conditions will be excluded:
(1) Patients with mental disorders or severe cognitive impairments who cannot participate in cooperation;
(2) Patients with a history of previous bleeding disorders, current use of warfarin or low-molecular-weight heparin;
(3) Patients who cannot receive acupuncture for reasons such as infections around the acupuncture points or allergy to acupuncture needles;
(4) Patients who have received acupuncture treatment in the past 6 months;
(5) Participants in other clinical trials that may interfere with the primary endpoint.
Intervention description {11a}
All participants will receive the electroacupuncture or sham electroacupuncture before the gastroscopy, then, they will undergo standard upper gastrointestinal endoscopy procedures. Patients in both groups will be discharged within 1 hour after the endoscopy, which includes a 30-minute observation period, a preference for future endoscopy assessment and blinding assessment. The acupuncture methods are described in Table 1.To maintain blinding. Patients will be asked to wear an eye-patch and receive treatment in a supine position in an isolated space with limited communication with the acupuncturist. The acupuncturist will disinfect the patient's skin with 75% alcohol cotton balls before treatment. Acupuncture treatment will last 30 minutes. After removing the needle, researchers will use a clean cotton ball to compress the acupoint to prevent bleeding. A total of 8 points will be used. Table 2 summarizes the acupoints and rationale.
Table 1
Treatment methods of electroacupuncture and acupoints
| |
EA group
|
SEA group
|
|
Acupoints
|
Hegu(LI4), Neiguan(PC6), Zusanli(ST36),Liangqiu(ST34)
|
Non-acupoints as shown in the Table 3
|
|
Depth of insertion
|
10 mm:LI4 PC6;30mm:ST36 ST34
|
Superficial acupuncture
|
|
Needle type
|
Steel needles (Wuxi Jiajian Medical Co. Ltd. Wuxi, China)
|
The same as EA group
|
|
Needle sensation
|
With de-qi sensation
|
Without de-qi sensation
|
|
Electric stimulation
|
Two pairs of needles:
|
Two pairs of needles:
|
| |
LI4–ST36 (bilaterally)
|
LI4–ST36 (bilaterally)
|
| |
Connected to CMNS6-1(Wuxi Jiajian Medical Device CO., China)
|
Connected to CMNS6-1(Wuxi Jiajian Medical Device CO., China)
|
| |
Deliver continuous wave-type low-frequency 2 HZ and current of 2mA
|
No electrical current delivered
|
|
EA electroacupuncture, SEA sham electroacupuncture
|
Table 2
Acupoint selection and rationale based on traditional Chinese medicine
|
Acupoint
|
Location
|
Traditional Chinese medicine indication
|
Suggested technique
|
|
LI4(hegu)
|
Dorsum of hand, at the level of the midpoint of the second metacarpal bone, between the first and second metacarpal bones
|
Relieve visceral pain
|
Needle perpendicular,0.5–1.0 cun
|
|
PC6(neiguan)
|
Palmar aspect of the forearm, between the tendons, 2 cun away from the transverse crease of the wrist
|
Reduce nausea and stomach pain
|
Needle perpendicular,0.5–1.5 cun
|
|
ST36(zusanli )
|
Antero-lateral leg, 1 middle-finger breadth next to the anterior crestof tibia, 3 cun under the depression lateral to the patellar ligament
|
Reduce nausea and stomach pain
|
Needle perpendicular,1–2 cun
|
|
ST34(liangqiu)
|
2 cun above the bottom of the patella, on the line between the anterior superior iliac spine and the lateral end of the bottom of the patella
|
Relieve stomach pain
|
Needle perpendicular,1–1.2 cun
|
Participants in the treatment group will receive EA treatment. The standard acupuncture method will be applied at 8 acupoints: bilateral Hegu (LI4), Neiguan (PC6), Zusanli (ST36) and Liangqiu (ST34). All acupoints were selected based on literature, clinical experience and acupuncture textbooks. The acupuncture needles will be disposable sterile needles made of stainless steel (0.25 × 40mm and 0.30 × 40 mm; Jia Jian, China). After insertion, needles will be manipulated using the lifting-thrusting and twirling technique. An electroacupuncture apparatus (CMNS6-1, Wuxi Jiajian Medical Device CO., China) will be connected to 2 pairs of needles (LI4, ST36 bilaterally) to deliver a continuous wave, low-frequency (2 Hz) and current of 2mA.
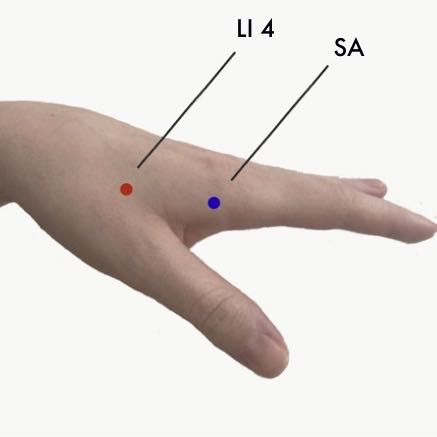
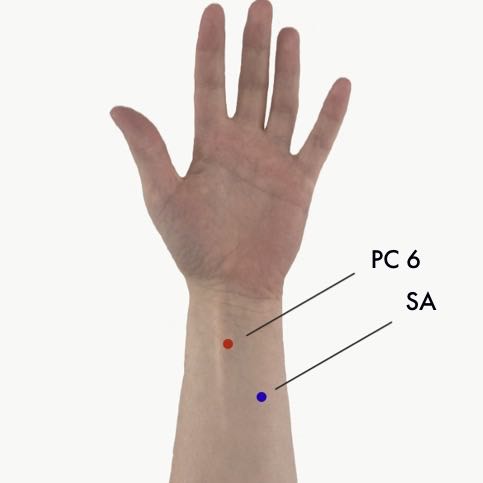
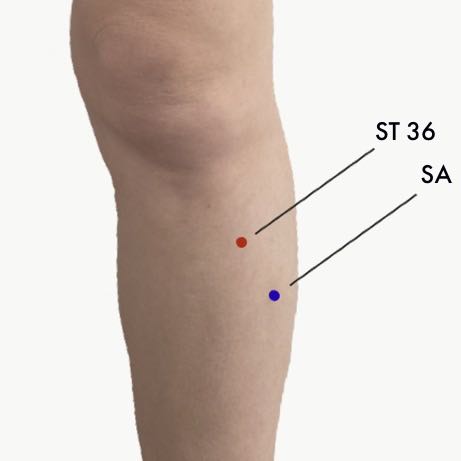
In the control group, we will use the same acupuncture needles as used in the EA group but repurposed as placebo needles. The acupuncturist will perform superficial acupuncture on the non-acupoints detailed in Table 3,and Picture1-4 show the location. All of the needles will be inserted using a needle tube to a superficial depth (2–3 mm) without invoking the sensation of “De-qi”. The electroacupuncture apparatus will be connected to 2 pairs of needles (LI4, ST36 bilaterally) for 30 min, but all indicators will be set to "0" to ensure no electrical current is delivered.
|
Table 3 Non-acupoints positioning
|
|
Acupoints
|
Non-acupoints
|
|
Hegu(LI4)
|
1 cun beside Zhigou(SJ6), between the sanjiao channel and the large intestine channel
|
|
Neiguan (PC6)
|
In the middle of the medial epicondyle of the humerus and the styloid process of ulna
|
|
Zusanli (ST36)
|
3 cun below Yanglingquan (GB34), between the gallbladder and bladder meridian
|
|
Liangqiu(ST34)
|
3 cun below Zhongdu(GB32),between the stomach meridian and the gallbladder meridian
|
Criteria for discontinuing or modifying allocated interventions {11b}
When acupuncture-related serious adverse reactions occur during the experiment or failure to complete the study for any other reasons. We will record the details in the report for the early termination of the study.
Strategies to improve adherence to interventions {11c}
At the beginning of the trial, participants will be informed of the experiment procedure again. They can report their personal feelings at any time during the study, and we will give corresponding feedback as appropriate to increase the interactivity and then improve adherence to interventions.
Relevant concomitant care permitted or prohibited during the trial {11d}
Patients cannot eat 8 hours before gastroscopy to ensure a fasting state.
Provisions for post-trial care {30}
At the end of the study, we will provide certain amount of subsidy to each subject.
Outcomes {12}
Primary outcome
A visual analogue scale (VAS) will be used to evaluate the patient’s level of discomfort, which is a line segment from 0 to 10, with 0 indicating low and 10 high discomfort. All patients will complete 4 detailed VAS at 30 minutes and 7 days post-procedure. The questionnaire will evaluate 4 areas of discomfort including nausea and vomiting, throat discomfort, bucking and agitation. The primary outcome is the average score of the 4 VAS scales
Secondary outcomes
All patients’ oxygen saturation (SpO2), heart rate (HR) and blood pressure (BP). measurements will be recorded prior to, during and post-procedure. Then, each patient’s ‘double product’ (DP) will be calculated at each point of the procedure, based on the systolic blood pressure (SBP) and heart rate (SBPⅹHR). DP is a useful prognostic tool for patients with poor cardiac function during exercise and rest, reflecting myocardial oxygen consumption and cardiac output during treadmill testing. A value of DP greater than 15,000 indicates cardiovascular stress. It is assumed that changes in cardiac output from baseline (preoperative) will reflect the level of stress experienced by patients undergoing the gastroscopy.
A six item short form of the State-Trait Anxiety Inventory (STAI-S6) and Amsterdam Pre-operative Anxiety and Information Scale (APAIS) will assess the degree of preoperative anxiety, postoperative anxiety and 7 days post-procedure. These questionnaires are quick and simple for participants to complete, which is advantageous in time-restricted studies.
Preference in a future endoscopy:
The questionnaire will ask patients whether they have undergone gastroscopy before, and then ask, “There are two options to choose when accept next gastroscopy, accept acupuncture before gastroscopy or do not accept acupuncture before gastroscopy.”
Before participants sign the informed consent form, they will be informed that acupuncture clinical trials may have potential adverse events such as bleeding, hematomas, fainting, bruising, ecchymoma and possible infection. All details of the adverse event will be recorded by the patients and doctors. Adverse events (AE) are rated as 1 (mild), 2 (moderate) or 3 (severe or medically significant). All details of AEs will be recorded in the Case Report Form (CRF). At the end of the trial, we will analyze the impact of all events.
After the gastroscopy procedure researchers will evaluate the success of the blinding by asking participants the following question: “what kind of treatment do you think you have received?” The options are: traditional acupuncture treatment; acupuncture-like simulation treatment; and uncertain. If participants do not choose “uncertain,” then the researcher will question the patient further for specific reasons.
Participant timeline {13}
The timing of intervention and data collection is detailed in Fig. 2.
Sample size {14}
In our pilot study, the discomfort VAS assessment at 30 minutes post-procedure was 4.8 (SD, 1.76) in the EA group and 6.3 (SD, 1.53) in the SEA group. We used PASS software to calculate that 50 patients would be needed to provide 90% power to detect a difference of discomfort VAS in 2 groups at a 2-sided significance level of 5%. If we assume that 20% of patients would be lost to follow-up, 60 would need to be enrolled.
Recruitment {15}
Participants will be recruited through hospital-based advertisements within the outpatient clinic and on the Shanghai Municipal Hospital of TCM website. Research assistants will screen the patients, obtain written informed consent, and assign them to either the EA or SEA group, receiving a traditional acupuncture or an acupuncture-like simulation treatment.
Assignment of interventions: allocation
Sequence generation {16a}
In this trial, we plan to use SPSS24.0 software to generate a random number table, which divides eligible participants into the EA group or SEA group with a 1:1 ratio.
Concealment mechanism {16b}
A random distribution card will be made and sealed with an opaque envelope. Participants will be informed that they have an equal chance of being assigned to the EA or SEA group before the trial.
Implementation {16c}
An independent researcher that blinded to the study protocol generate the allocation sequence. Another researcher will give the opaque envelope to acupuncturist according to the timing sequence of participant registration for the trial.Then, acupuncturist open the envelope to perform corresponding acupuncture operation.
Assignment of interventions: Blinding
Who will be blinded {17a}
This is a single-blinded (patient-assessor-blinded) study. To ensure that participants are blind, they will be treated in an isolated space and be required to wear blindfolds. Only the acupuncturist who performs the treatment will know the group assignment at the time of treatment. Gastroenterologists, data analysts and statisticians will remain blinded.
Procedure for unblinding if needed {17b}
Unmasking is not needed.
Data collection and management
Plans for assessment and collection of outcomes {18a}
We will timely record the evaluation results in the CRFs.
Plans to promote participant retention and complete follow-up {18b}
Patients came to the hospital one week after gastroscopy to get the result of pathological organization,We followed up at this time point.At the end, gave a certain transportation subsidy.
Data management {19}
Patient characteristics will be recorded in the CRFs and stored in the researcher's office. The clinical trial management platform ResMan will be used to manage the raw data. The raw data will be collected by assessors who are blinded to the group assignment and repeated input methods will be used to ensure that the entered data is correct. Before the platform is officially launched, it will be tested and the users will be trained. After the platform is officially launched, the database will be locked with a password, which only be known by relevant personnel. The clinical director will oversee the work of the clinical trial center at least once a month.
Confidentiality {27}
All the documents and materials related to this will be kept strictly confidential. Only when principal Investigator allowed will the documents promulgated to the third parties. We protect the privacy of participants' personal medical information within the sphere permitted by law. The staff in this study is also bound by this agreement.
Plans for collection, laboratory evaluation and storage of biological specimens for genetic or molecular analysis in this trial/future use {33}
Not applicable, this trial does not have biological specimens.
Statistical methods
Statistical methods for primary and secondary outcomes {20a}
The independent statistician is responsible for the statistical analysis with spss24.0 software. All data will be analyzed in terms of intention to treat (ITT) principle, including data from participants who withdraw during the trial. In the statistical analysis, measurement data between the two groups will be analyzed with the t-test, and rank- sum test, while categorical data will be analyzed with χ2 test. Data will be recorded as mean ± standard deviation or median (first quartile, third quartile). The significance level used for statistical analysis will be two-sided with confidence intervals at the 95% level.
Interim analyses {21b}
Not applicable.
Methods for additional analyses (e.g. subgroup analyses) {20b}
Not applicable.
Methods in analysis to handle protocol non-adherence and any statistical methods to handle missing data {20c}
We will adopt ITT principle to reduce deviation. The missing data will be substituted into the subjects' baseline data for final data analysis.
Plans to give access to the full protocol, participant level-data and statistical code {31c}
The data sharing will be conducted in accordance with the regulatory requirements.
Oversight and monitoring
Composition of the coordinating centre and trial steering committee {5d}
In order to control the quality of the clinical trial, the whole process of the trial will be conducted under the supervision of a qualified clinical trial expert in Shanghai Municipal Hospital of Traditional Chinese Medicine. The Clinical Research Center for Drugs of Shanghai University of Traditional Chinese Medicine will conduct the data monitoring. When problems occur in the trial, the center has the right to make the final decision to terminate the trial if necessary. Any changes will be notified in writing to all participants in the trial after approval by the ethics committee. The principle investigator will be fully responsible for conducting the trial and will make any final decisions.
Adverse event reporting and harms {22}
We will record the adverse events such as bleeding, hematomas, fainting, bruising, ecchymoma and possible infection, and analyzed.
Frequency and plans for auditing trial conduct {23}
We will audit every three months,any modification that may have an impact on the study, potential benefit to patients, or affect patient safety, including changes of the study objective, study design, patient population, sample size, study procedure or serious adverse events will be reported to the Committee. This will be decided jointly with the monitoring Committee, the Clinical Research Center of Drugs and approved by the Ethics Committee.
Dissemination plans {31a}
The publication of the outcomes of this study will provide baseline data. The outcomes may be presented at conferences, symposiums, teaching classes, etc., if applicable.
{kind=link}
{kind=link}
{kind=link}
{kind=link}