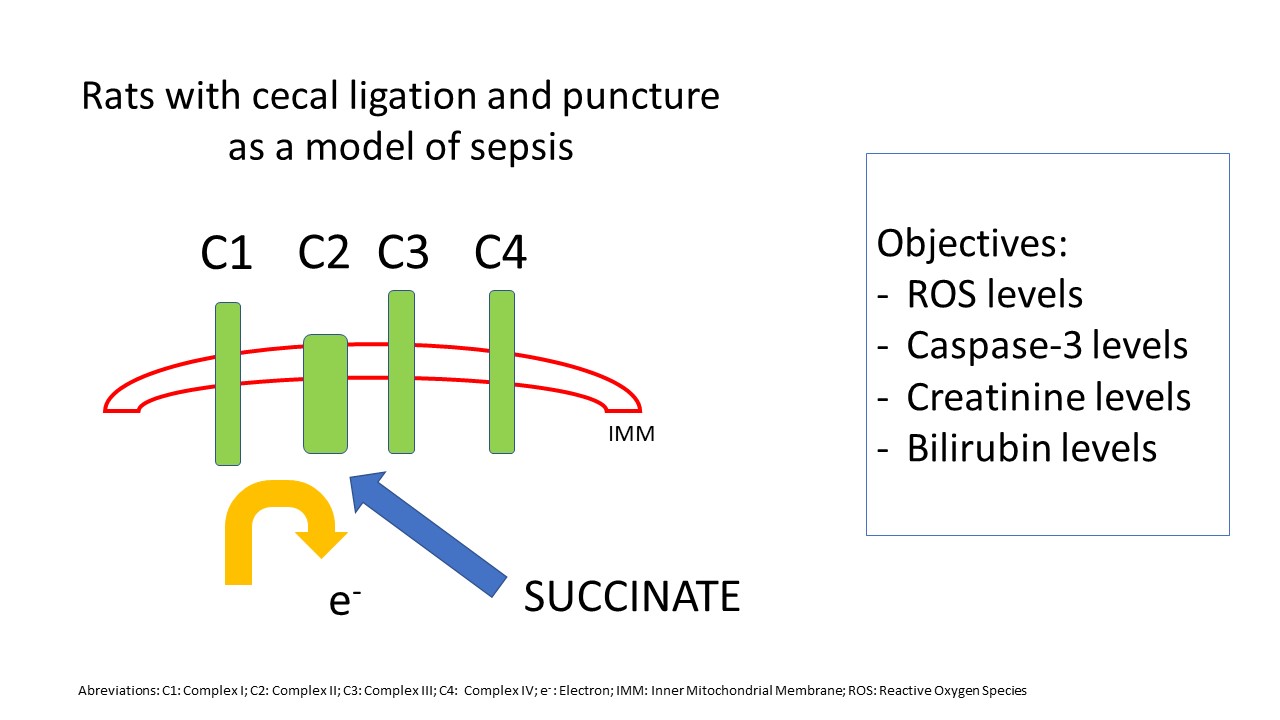
The aim of the administration of succinate to the rats was to provide a substrate for Complex II of the electron transport chain and reducing ROS production. Thus, it was determined that systemic ROS levels are elevated in septic rats when compared with the Control group and that the administration of parenteral succinate reduces the production of these species in septic rats. In contrast, parenteral succinate administered in rats that did not undergo cecal ligation and puncture does not cause any changes regarding the Control group, suggesting that succinate does not affect non-septic rats. In previous studies, it has been documented that succinate reduces serum ROS levels, but it does not improve creatinine levels in septic rats [22], but the present research aimed to find a correlation between serum ROS levels and serum apoptosis markers, also, the correlation between apoptosis markers and organ dysfunction markers as bilirubin and creatinine.
There are controversial publications regarding succinate levels in pathological situations, and one of them is hypoxia-reoxygenation. Chouchani et al. demonstrated an accumulation of succinate during hypoxia-reoxygenation cycles in mice [34]. Through various tests, glucose, palmitate, glutamate, and GABA do not contribute to its accumulation. Instead, the cause of the accumulation would be fumarate. On the other hand, Wijemars et al. analyzed biopsies of transplanted kidneys and observed a drop in tissue succinate accumulation [35]. However, hypoxia-reoxygenation is not the only pathophysiological mechanism in sepsis.
Several studies evidenced changes in the processes that occur within the mitochondria during sepsis, among which the electron transport chain is affected. Literature is not conclusive regarding the activity rank of the different complexes at this level. Lorente et al. demonstrated decreased action in the electron transport chain in Complex IV [36], while Brealey et al. found decreased Complex I activity but found no differences in Complexes II, III y IV [37–39]. Furthermore, the same group demonstrated that the activity of Complexes II and III remained unchanged both in the muscles and the liver in septic rats [37–39]. Contrariwise, in those organs, Complex I activity seemed to increase with the severity of sepsis in rats.
In another study done on septic rats, using the cecum ligation and puncture technique, the infusion of dimethyl succinate improved the survival of the rats [20]. On the other hand, it was demonstrated that, in rats that were administered LPS, dimethyl succinate infusion improved ATP levels and the ATP/ADP ratio, which would suggest a recovery in the activity of the electron transport chain [21]. A different study determined that Complex I activity was decreased in the soleus muscle of rats with moderate/severe sepsis caused by the intraperitoneal administration of a fecal matter preparation. In contrast, there were no changes in Complex II activity in control group rats. In addition, the administration of malate and glutamate (as Complex I substrates) and succinate (as Complex II substrate) improved muscle oxygen consumption compared with the administration of malate and glutamate alone. Furthermore, this improvement was more pronounced in rats with moderate/severe sepsis than in rats with mild sepsis [19].
Creatinine levels increased by 22% in septic rats, but the differences were not statistically significant compared with the Control group. In contrast, serum creatinine levels in septic rats with parenteral succinate did not decrease compared with septic rats without treatment, although they showed significant differences compared with the Control group. Creatinine is a late marker of kidney failure, and a marker such as NGAL, which would give an early account of the damage and show significant differences among the different groups, was not used [40–42].
Lastly, there was no correlation between ROS levels and creatinine, total bilirubin, and urea levels. This observation suggests that there would be no pathophysiological association between ROS levels and organ failure. This data contrasts with the previous study, where there was a correlation between ROS levels and serum creatinine levels. As previously stated, the cause and pathophysiology of MOF is multifactorial, which is probably one of the causes for the lack of correlation among the variables mentioned above. That is to say that the increase in creatinine levels would be determined by ROS status and other previously described pathophysiological mechanisms, such as pH, coagulation, endothelial, and microcirculation alterations, among others.
Total bilirubin levels in non-septic rats did not increase with succinate administration compared with the Control group. In addition, there were no differences in total bilirubin levels in septic rats with and without treatment with succinate. The only reference found in the literature regarding the effect of succinate on the liver of septic rats states that succinate infusion improves the concentration of β-hydroxybutyrate, increases ATP concentration in hepatocytes, and glucose oxidation, and also decreases the lactate/pyruvate ratio [21].
Since Caspase-3 is an apoptosis marker commonly used in the literature [12,43–46], it was measured to determine apoptosis levels [47], both at the tissue and serum levels. The aim of measuring serum Caspase-3 was to determine whether it could indicate tissue apoptosis.
There were no differences in serum Caspase-3 levels among the 4 groups, nor in tissue Caspase-3 levels in the liver and the kidney among the 4 groups. It is known that, in animal models of sepsis, apoptosis levels in different organs are increased. For example, in a study done on rats exposed to LPS, it was observed that the activity of Caspases-3, -8, and -9, as well as TNF-α levels, increased in the left ventricle [48]. On the other hand, rats that underwent cecal ligation and puncture and were subsequently euthanized at different times showed an increase in renal apoptosis, measured using the TUNNEL technique, with a peak at 6 hours. Furthermore, renal apoptosis measured by cytokeratin 18 fragment M30 had 2 peaks, one at 6 hours and another at 48 hours [49]. In this study, the determination of markers was done at 24 hours and 48 hours, respectively. The mortality of the rats was very high and could have altered the results and, at 6 hours, it could be an early measurement, and there probably would have been no differences in serum ROS levels. Therefore, the difference between the results obtained in this research and those obtained in the above-mentioned publications could be due to the kinetics of elevation in serum of those markers.
On the other hand, immunohistochemical studies show that, in sepsis, there is a higher degree of lymphocyte and digestive tract cell death, whereas, in the kidney, liver, and lungs, cell death is lower [45,50]. In addition, in a study done on sheep (with Escherichia coli infusion), it was observed that there was no increase in apoptosis markers in the kidney in septic animals. However, in animals that recovered from sepsis (the infusion of bacteria was suspended, and gentamicin was administered) those markers increased in the kidney [51]. These findings coincide with the results presented in this study since the animals were septic when taking the sample.
There was no correlation between tissue Caspase-3 levels and creatinine or total bilirubin levels either. This finding would indicate that serum markers of organ failure are not associated with levels of tissue apoptosis, at least within the first hours of the event. As described in the paragraph above, as apoptosis tissue markers do not increase, this could cause the lack of increase in serum and the absence of correlation between apoptosis markers and biochemical parameters of organ failure. In addition, there was no correlation between serum Caspase-3 levels and serum ROS levels. In a previous work with septic patients, we showed that septic patients have higher levels of Caspase-3 but not higher levels of serum ROS and both markers didn´t correlate [52]. This conclusion could be since both processes are not related or do not co-occur in sepsis.
The main limitations of the study are the single time measurement of ROS and apoptosis markers which did not allowed to determinate if the lack of correlation was both processes are related but not synchronic. The other limitation is that renal function was determinated with creatinine but not N-GAL. The main strength is that serum ROS were measured and not oxidative stress, and it was correlated with apoptosis markers also with kidney and liver damage markers.
{kind=link}