Identification of optimized METamp detection parameters using in silico analysis
We first determined the most appropriate parameters for NGS-based METamp detection using ifCNV. We conducted 2,000 simulations for each CNR threshold value (ranging from 0.5 to 2.4, with an increment of 0.1) and contamination value (ranging from 0.017 to 0.031 with an increment of 0.01) (Fig. 1a). This process yielded a total of 750,000 distinct simulations using a training set of over 2,000,000 samples. We calculated the binary classification indicators for each CNR threshold and contamination value, aiming to maximize the F-score. The optimal values were identified as a CNR threshold of 1.5 and a contamination value of 0.028 (Fig. 2a).
Using these optimized parameters, we evaluated the ability of the NGS-based METamp detection method to accurately stratify samples. We conducted an additional set of 7,000 simulations, increasing the number of reads on the MET amplicons in the synthetic datasets by factors ranging from 2 to 5. Subsequently, we calculated the corresponding CNR using ifCNV for each simulation. Interestingly, Pearson correlation analysis revealed a strong correlation (exceeding 0.99) between expected and observed ratios (Fig. 2b). In addition, despite a slight under-evaluation in the observed CNR, the stratification of the samples into Low-, Medium-, and High-amplification groups exhibited 100% accuracy (Fig. 2b).
In vivo validation of optimized METamp detection parameters
Using these established parameters, we next evaluated the NGS-based METamp detection and stratification method on a validation set of 72 NSCLC samples with a tumor cell percentage of 20% or higher (Fig. 1b). We assessed the METamp status using IHC, ddPCR, and NGS, and compared the results obtained with those of the current gold standard approach FISH. IHC exhibited a perfect Se but a low Sp of 0.19, revealing a considerable number of FPs. The ddPCR analysis on the other hand, when possible (25 samples), gave a Se of 0.83 and Sp of 0.77. Our NGS-based METamp detection method had a Se of 0.91 and Sp of 0.98, with only one FP and 2 FN when compared to the FISH results (Table 1 and Supplementary Table S2).
Next, we evaluated the ability of the NGS-based METamp detection method to accurately stratify patients into groups based on amplification levels. We utilized FISH as the reference standard and evaluated the performance of the NGS-based method for METamp stratification relative to this reference. Among the 20 samples identified as amplified by both FISH and NGS, the NGS-based stratification achieved global Se and Sp of 0.93 and 0.97, respectively (Table 1). NGS misclassified only one sample as belonging to the Medium-amplification group whereas FISH classed the sample in the High-amplification group (Supplementary Table S2). Of note, ddPCR-based classification, performed on 11 samples, gave a Se and Sp of 0.78 and 1, respectively (Table 1).
Table 1
Binary classification indicators of METamp detection and stratification. METamp status and level stratification of the samples was determined using FISH as follows: MET-to-CEP7 ratios between 1.8 and 2.2 are classified as Low-amplification, those between 2.2 and 4 as Medium-amplification, and those over 4 as High-amplification. IHC, immunohistochemistry; ddPCR, digital droplet PCR; NGS, next-generation sequencing; TP, true positive; TN, true negative; FP, false positive; FN, false negative; Se, sensitivity; Sp, specificity; NA, not applicable.
| | | IHC | ddPCR | NGS |
| METamp detection | | TP | 18 | 10 | 20 |
| | TN | 3 | 10 | 49 |
| | FP | 13 | 3 | 1 |
| | FN | 0 | 2 | 2 |
| | Se | 1.00 | 0.83 | 0.91 |
| | Sp | 0.19 | 0.77 | 0.98 |
| METamp level stratification | Low (n = 5) | TP | NA | 1 | 5 |
| TN | NA | 9 | 15 |
| FP | NA | 0 | 0 |
| FN | NA | 1 | 0 |
| Se | NA | 0.50 | 1.00 |
| Sp | NA | 1.00 | 1.00 |
| Medium (n = 10) | TP | NA | 5 | 10 |
| TN | NA | 5 | 9 |
| FP | NA | 0 | 1 |
| FN | NA | 1 | 0 |
| Se | NA | 0.83 | 1.00 |
| Sp | NA | 1.00 | 0.90 |
| High (n = 5) | TP | NA | 3 | 4 |
| TN | NA | 8 | 15 |
| FP | NA | 0 | 0 |
| FN | NA | 0 | 1 |
| Se | NA | 1.00 | 0.80 |
| Sp | NA | 1.00 | 1.00 |
| Global (n = 20) | Se | NA | 0.78 | 0.93 |
| Sp | NA | 1.00 | 0.97 |
Evaluation of the NGS-based METamp detection method as a relevant screening assay
We next applied the NGS-based METamp detection method to an independent retrospective cohort encompassing 1,932 NSCLC patients (Fig. 1c). Among these patients, 62 (3.2%) tested positive for METamp, with 16 having undergone EGFR-TKI treatment prior to the analysis. The remaining 46 patients had not received any treatment prior to the NGS analysis and were therefore classified as de novo cases. Stratification of these de novo cases based on METamp levels into three distinct groups resulted in: 22 (47.8%) in the Low- (1.5 ≤ CNR < 2.2); 17 (37.0%) in the Medium- (2.2 ≤ CNR < 4); and 7 (15.2%) in the High- (CNR ≥ 4) amplification groups, respectively (Table 2). The three amplification groups showed no significant differences with regards to clinicopathological data except for the PD-L1 TPS were the High-amplification group was enriched in negative (< 1%) patients (Table 2). Although not statistically significant (p = 0.07), it is noteworthy that the High-amplification group displayed advanced stage disease, exclusively comprising stage IV patients, while the other groups also included stage III patients (45% and 29% for the Low- and Medium-amplification groups, respectively) and one stage II patient in the Low-amplification group.
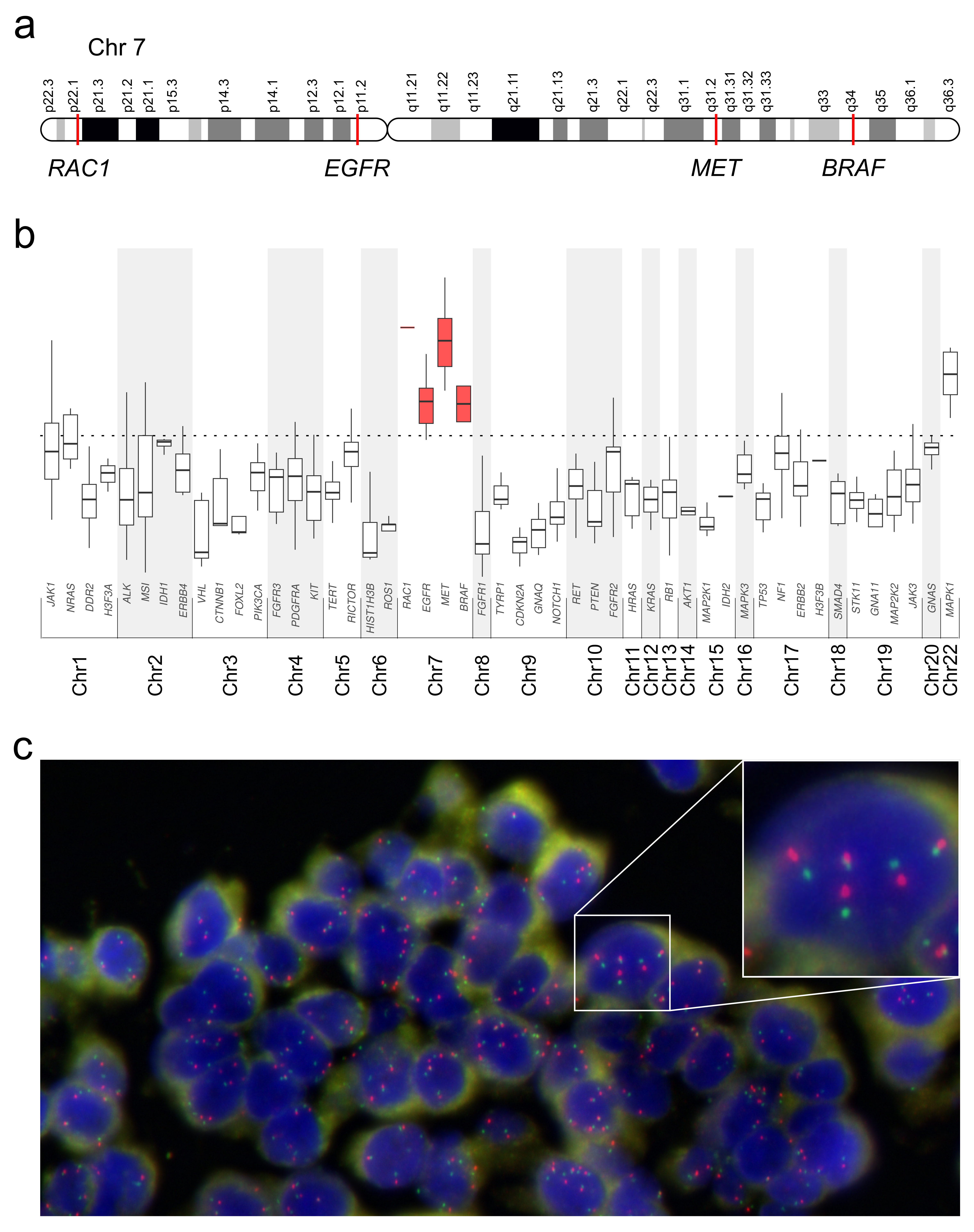
We next determined the prevalence of co-occurring molecular alterations in the cohort of 46 de novo METamp patients (Fig. 3). Within the subgroup of patients with TP53 in their sequencing panel (n = 33), 29 (87.9%) exhibited a partially or non-functional TP53 mutation, in accordance with the International Agency for Research on Cancer guidelines (23). Five (10.9%) of the de novo METamp patients also harbored a concurrent targetable alteration defined as ESCAT Tier I by the European Society for Medical Oncology (ESMO) (24) (Fig. 3 and Supplementary Table S3). These included 2 patients with an EGFR-activating alteration, 2 with a KRASG12C variant and 1 with a variant on MET causing the skipping of exon 14. Of note, we detected all these alterations in tumor samples from patients stratified into the Low-amplification group. A further 17 samples (37.0%) showed other concurrent alterations classified as ESCAT Tier II/III/IV/V/X: 5 (10.9%) had a variant on STK11; 4 (8.7%) on CDKN2A; 3 (6.5%) on BRAF; 2 (4.35%) on MET; 2 (4.35%) on FGFR2; 1 (2.2%) on KRAS; 1 (2.2%) on KIT; 1 (2.2%) on ALK; and 1 (2.2%) on PIK3CA (Fig. 3 and Supplementary Table S3). Interestingly, as previously reported, 6 out of 7 patients in the High-amplification group exhibited only TP53 alterations, suggesting that METamp is the primary oncogenic driver in these cases (25).
Table 2
Clinicopathological characteristics of the de novo METamp patients of the retrospective cohort. ap-value (χ2 test) was considered significant when p < 0.05. NS, not significant. TPS, tumor proportion score.
| | | | de novo METamp groups | |
| | Total | | Low | Medium | High | pa |
| n | 46 | | 22 | 17 | 7 | |
| Age, y | | | 63.8 (47–83) | 57.9 (30–75) | 58.9 (39–67) | |
| Sex | | | | | | |
| Male | 32 | | 14 (64%) | 11 (65%) | 7 (100%) | NS (0.16) |
| Female | 14 | | 8 (36%) | 6 (35%) | 0 (0%) | |
| Smoking status | | | | | | |
| Ever | 35 | | 14 (64%) | 15 (88%) | 6 (86%) | NS (0.48) |
| Never | 1 | | 1 (5%) | 0 (0%) | 0 (0%) | |
| Unknown | 10 | | 7 (32%) | 2 (12%) | 1 (14%) | |
| Stage | | | | | | |
| II-III | 15 | | 10 (45%) | 5 (29%) | 0 (0%) | NS (0.07) |
| IV | 31 | | 12 (55%) | 12 (71%) | 7 (100%) | |
| Brain metastasis | | | | | | |
| Yes | 11 | | 6 (27%) | 4 (24%) | 1 (14%) | NS (0.75) |
| No | 33 | | 15 (68%) | 12 (71%) | 6 (86%) | |
| Unknown | 2 | | 1 (5%) | 1 (6%) | 0 (0%) | |
| Histological type | | | | | | |
| Adenocarcinoma | 39 | | 20 (91%) | 14 (82%) | 5 (71%) | NS (0.43) |
| Others | 7 | | 2 (9%) | 3 (18%) | 2 (29%) | |
| Treatment | | | | | | |
| Chemotherapy | 29 | | 15 (68%) | 11 (65%) | 3 (43%) | NS (0.26) |
| Immunotherapy | 27 | | 15 (68%) | 11 (65%) | 1 (14%) | |
| EGFR-TKI | 2 | | 2 (9%) | 0 (0%) | 0 (0%) | |
| Crizotinib | 1 | | 0 (0%) | 1 (6%) | 0 (0%) | |
| No treatment | 5 | | 2 (9%) | 1 (6%) | 2 (29%) | |
| Unknown | 2 | | 0 (0%) | 1 (6%) | 1 (14%) | |
| EGFR mutation status | | | | | |
| Negative | 44 | | 20 (91%) | 17 (100%) | 7 (100%) | NS (0.32) |
| Positive | 2 | | 2 (9%) | 0 (0%) | 0 (0%) | |
| TPS PD-L1 | | | | | | |
| > 1% | 32 | | 17 (77%) | 12 (71%) | 3 (43%) | 0.04 |
| < 1% | 9 | | 2 (9%) | 3 (18%) | 4 (57%) | |
| Unknown | 5 | | 3 (14%) | 2 (12%) | 0 (0%) | |
Clinical implications of NGS-based METamp detection and stratification
We then explored the correlation between de novo METamp level and patient outcomes to evaluate its potential prognostic significance in terms of OS. Groups showed significant differences (log-rank test, p < 0.001) (Fig. 4a), i.e. patients from the Low-amplification group displaying a more favorable outcome (median OS: 35.9 months) than those from the Medium- (median OS: 14.3 months) or from the High-amplification groups (median OS: 3.3 months). No prognostic value was observed for the other clinical parameter evaluated, even if PD-L1 TPS and the stage tended to be significant (p = 0.08 and 0.06, respectively, Table 3). Prognostic factors with a p < 0.1 in univariate analysis were subsequently entered in a multivariate Cox model, and only the prognostic significance of METamp level persisted in the model.
Due to the limited number of patients in the Medium- and High-amplification groups, we merged them to evaluate patients’ response to treatment. Interestingly with regards to PFS, we observed a reduced response to chemotherapy in patients from the Medium/High-amplification groups compared to those in the Low-amplification group (log-rank test, p = 0.001) (Fig. 4b and Table 3). Of note, we found no statistically significant difference in response to immunotherapy between the two groups (log-rank test, p = 0.745) (Fig. 4c), in accordance with previously published data (26).
Table 3
Univariate and multivariate analysis of the prognostic value of METamp. aHR, Hazard ratio. b95% CI, 95% confidence interval. cp was considered significant when p < 0.05. NS, not significant. ND, not done. TPS, tumor proportion score.
| | | | | Univariate (Log-rank test) | | Multivariate Cox proportional hazard analysis |
| | | | Number of samples | HRa | 95% CIb | Pc | | HR | 95% CI | P |
| Overall Survival | | | | | | | | | |
| | Brain metastasis (No; Yes) | | 44 | 0.757 | 0.283–2.025 | NS (0.58) | | | | ND |
| | PD-L1 TPS (< 1; > 1) | | 41 | 0.481 | 0.205–1.127 | NS (0.08) | | | | NS |
| | Stage (II + III; IV) | | 46 | 2.317 | 0.931–5.762 | NS (0.06) | | | | NS |
| | METamp level (Low; Medium; High) | | 46 | | | < 0.001 | | 3.819 | 2.179–6.794 | < 0.001 |
| | | Low; Medium | | 2.542 | 1.019–6.339 | | | | | |
| | | Medium; High | | 5.946 | 1.835–19.267 | | | | | |
| | | Low; High | | 12.229 | 3.019–49.537 | | | | | |
| PFS under chemotherapy | | | | | | | | | |
| | Brain metastasis (No; Yes) | | 28 | 0.945 | 0.310–2.885 | NS (0.92) | | | | ND |
| | TPS PD-L1 (< 1; > 1) | | 26 | 0.463 | 0.166–1.291 | NS (0.13) | | | | ND |
| | Stage (II + III; IV) | | 29 | 1.356 | 0.564–3.260 | NS (0.49) | | | | ND |
| | METamp level (Low; Medium + High) | | 29 | 6.326 | 1.934–20.693 | 0.001 | | 6.326 | 1.934–20.693 | 0.001 |
| PFS under immunotherapy | | | | | | | | | |
| | Brain metastasis (No; Yes) | | 27 | 0.269 | 0.061–1.175 | NS (0.06) | | | | ND |
| | TPS PD-L1 (< 1; > 1) | | 25 | 0.702 | 0.246–2.008 | NS (0.51) | | | | ND |
| | Stage (II + III; IV) | | 29 | 0.932 | 0.378–2.298 | NS (0.88) | | | | ND |
| | METamp level (Low; Medium + High) | | 29 | 0.864 | 0.356–2.097 | NS (0.74) | | | | ND |
{kind=link}