We report long term results (mean follow-up higher than 8 years) of 89 patients with initial BMI ≥ 50kg/m2 submitted to RYGB or SG. All patients had at least 5 years follow-up after surgery.
The outcomes were reported using a comprehensive and standardized score. The Swiss-Finnish Bariatric metabolic outcome score (SF-BARI Score) [11] was developed by an international team led by two renowned and experienced bariatric surgeons, from the merged data from two large randomized clinical trial [12, 13]. The SF-BARI Score considers different outcomes after surgery: weight loss, co-morbidities improvement, complications and, optionally, quality of life. The easy-to-use scoring system, based on a simple website without any patient identification, provides a continuous and categorical variable that sums all the relevant information regarding outcomes after MBS. We consider it an excellent tool to standardize reports of treatment outcomes and very useful to compare results within and between different centers around the world.
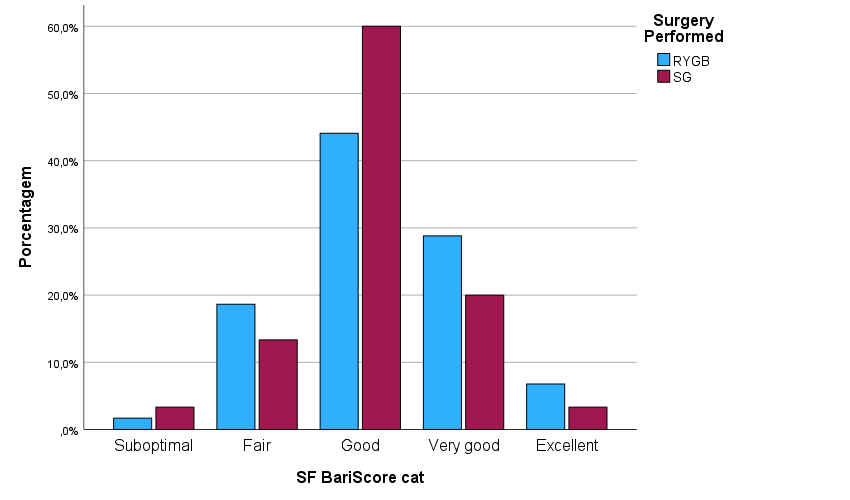
In our study, at last follow-up available, 81% of patients achieved good, very good or excellent results according to SF-BARI Score. These findings reflect that 85% patients had %TWL > 20, and 72% patients had %EWL > 50, which are commonly referred as markers of adequate weight loss after MBS. As expected, we also observed a high rate of co-morbidities improvement and a low complication rate.
Although most patients achieved a “good” or better category according to the SF-BARI Score in the long term, fewer than 35% attained a BMI < 35 kg/m2, and less than 3.5% were classified as non-obese (BMI < 30 kg/m2). A BMI above 50 kg/m2 has been associated to reduced weight loss outcomes after MBS [14, 15], demanding adjustments in the criteria for satisfactory weight loss in this population. Consistent with other authors [10], a BMI < 40 kg/m2 may be considered a satisfactory weight loss outcome at long-term follow-up. In our series, 72% of patients achieved a final BMI below 40 kg/m2, aligning more closely with the outcomes obtained by the SF-BARI Score.
As previously discussed, the comprehensive evaluation of MBS outcomes must incorporate various factors beyond weight loss alone. Nevertheless, these findings also highlight the need for more effective strategies to achieve better weight loss results. This may involve considering more “aggressive” surgical options or two-step approaches, combining pharmacotherapy or endoscopic therapy with subsequent MBS. Some studies suggest that surgeries such as One-Anastomosis Gastric Bypass (OAGB) [16], Single Anastomosis Duodenal-Ileostomy with Sleeve (SADI-S) [17], or biliopancreatic diversion with duodenal switch (BPD-DS) [18] may be more effective for patients with BMI ≥ 50kg/m2, although probably with higher long term nutritional complications. There is a paucity of data on long-term outcomes of these procedures in patients with BMI ≥ 50 kg/m2.
Patients should be thoroughly informed about the potential challenges in achieving an optimal weight even after undergoing MBS. It is also important to emphasize that this limitation may restrict access to body contouring surgeries, as most plastic surgeons set a BMI threshold of 28–30 kg/m2 for such procedures due to the increased risk of wound healing complications [19]. Comprehensive counselling, careful management of expectations, and clear communication regarding objectives, risks and benefits of MBS are essential for all patients, particularly those with a BMI ≥ 50 kg/m2.
Recent systematic review and meta-analysis [5, 6] comparing long term outcomes of RYGB and SG in patients with BMI ≥ 50kg/m2, suggested that RYGB leads to improved outcomes at 12 months, but no difference was found at 24 or at 36 months. There are conflicting published data regarding which surgery may be the best for patients with BMI ≥ 50kg/m2. In our study, the type of surgery (RYGB or SG) did not significantly impact the SF-BARI Score or its components. Nonetheless, we observed that RYGB consistently demonstrated higher mean weight loss, greater resolution of comorbidities, higher percentage of patients achieving a final BMI < 35 kg/m2 and higher mean SF-BARI Score. These differences, however, did not achieve statistical significance, which may be explained by the small population sample. As for surgical complications, some studies report that RYGB is related to a higher rates of reoperation and readmission at 30 and 90 days [20], but this data was inconsistent with our findings and other studies [21, 22]. It seems that both surgeries have a high safety profile even in patients with BMI ≥ 70kg/m2 when performed by experienced teams [23].
We examined the statistical association of SF-BARI Score with variables such as age, gender, diabetes and initial BMI. Significant associations were found only with age. When categorizing age into younger (18–39 years) and older (40–65 years) groups, significant differences were identified in the SF-BARI Score in the long term after bariatric surgery, particularly regarding the improvement in comorbidity scores. The analysis of continuous variables confirmed these findings, but the correlation strength was low. It must be noted that the higher scores observed in the young population were mostly explained by the improvement of comorbidities rather than %TWL or surgical complications. Some studies suggests that older age may be considered an additional risk factor for post-operative complications [24], particularly in this group of patients with BMI ≥ 50kg/m2 who typically present with more severe associated diseases, reduced functional reserve and an overall higher risk of anesthetic complications.
Despite its utility, the SF-BARI Score presents some limitations that may affect its interpretation and clinical application. A primary limitation is the potential overlap of different outcomes. For example, a patient who experiences complication such as Petersen's hernia, which is promptly resolved via laparoscopic surgery with minimal long-term impact on quality of life, may nonetheless exhibit a significant change in score. Additionally, the SF-BARI score does not account for nutritional complications, which are not uncommon following MBS and can profoundly influence a patient’s health [25]. Another limitation is the omission of the patient’s goal of obesity improvement, with far-reaching implications such as the pivotal role of MBS as a bridge to other surgeries (eg. orthopedic or transplantation). The absence of this consideration prevents the score from fully capturing the patient's progress toward a critical outcome. Furthermore, the SF-BARI score is restricted to evaluating a specific set of comorbidities — diabetes, dyslipidemia, hypertension, and obstructive sleep apnea – thereby excluding other significant associated diseases that may play a vital role in determining the overall success of surgery and the patient's long-term health. We recognize that SF-BARI Score aimed to provide a simple and intuitive tool that could not encompass the many complexities of MBS outcomes.
We must acknowledge some limitations in our study. We had a small number of patients, especially those with a BMI greater than 60 kg/m2 (only 6 patients, 6.7%). These patients with very high BMI are often lost to follow-up, which could be attributed to various factors such as unsatisfactory outcomes leading to loss of motivation, greater psychosocial sequelae [26] or mobility difficulties. Thus, the selection criteria requiring available follow-up data above five years likely selected the most motivated patients who continued in follow-up, and probably those with more satisfactory results. Another potential source of bias is that we did not analyse the use of non-surgical treatments that patients might have undergone during the follow-up period. There is also some admitted heterogeneity in our population, as some patients underwent intragastric balloon placement before surgery. We did not integrate the quality of life in the score, so no conclusions could be made about this very relevant topic.
{kind=link}