The therapeutic effect of tocilizumab remains controversial. We aimed to evaluate whether tocilizumab might be beneficial in COVID-19 patients. We searched PubMed, Embase and Cochrane library from inception to June 23, 2020. Summary estimates of overall response rate (ORR) and all-cause death rate in all patients were analyzed. This study was registered with PROSPERO (CRD42020191313). We included data from 28 articles including 991 COVID-19 patients who underwent tocilizumab administration. The pooled ORR was 72% (95% CI, 66-79%) and pooled all-cause death rate was 16% (95% CI, 11-22%). The optimal timing of administration was the 7.15 day from the symptom onset and with the lowest death rate of 13.11%. 562 patients were defined as with severe infection, and the pooled ORR was 78% (95% CI, 70-85%). The pooled ORR of 56 organ transplantation recipients was 53% (95% CI, 26-78%), which was lower than non-transplant patients [75% (95% CI, 69-81%)]. Nearly all studies confirmed the safety of tocilizumab administration. Tocilizumab improves the clinical outcome of COVID-19 patients, especially in severe cases, and the optimal timing of administration may provide the guidance for management. However, tocilizumab may be used with caution in solid transplant recipients for the suboptimal efficacy.
Systematic Review
Efficacy and safety of tocilizumab in COVID-19 patients: A Meta-Analysis
https://doi.org/10.21203/rs.3.rs-50446/v1
This work is licensed under a CC BY 4.0 License
Version 1
posted
You are reading this latest preprint version
Since December 2019, the world has been facing the pandemic of a novel coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). As of 17th June, the pandemic has affected over 8 million individuals and caused more than 440000 deaths worldwide, posing great threat to the global health and economy.1 The need for effective treatment is urgent. The signs and symptoms of COVID-19 patients vary from mild to severe, such as fever, cough, dyspnea, and some people may even experience pneumonia, acute respiratory distress syndrome (ARDS) and multi-organ failure.2 As such, the management may be suggested to provide supportive care for patients with non-severe disease while additional antiviral therapies for severe patients. However, the optimal therapeutic approaches has not reached a conclusion.
Although the pathophysiology of COVID-19 remains to be fully elucidated, accumulating evidence suggests that cytokine release syndrome (CRS) plays a key role in the severe manifestations of the disease.3 CRS refers to a systemic inflammatory response characterized by uncontrolled and excessive secretion of inflammatory cytokines including IL-6.4 Higher plasma level of IL-6 is often associated with more severe disease in COVID-19 patients.5 In addition, several retrospective studies have identified elevated level of IL-6 as a negative prognostic factor for survival.6,7 Therefore, in the situation where effective vaccines and antiviral therapies are lacking, the existing therapeutic, tocilizumab, that blocks IL-6 pathway was put forward and regarded as a potential treatment to reduce the mortality of COVID-19 patients. Tocilizumab is a humanized monoclonal antibody that targets IL-6 receptor. It has been widely used in patients with rheumatoid arthritis, juvenile idiopathic arthritis, and giant cell arteritis8. In 2017, FDA approved it for the treatment of severe or life-threatening chimeric antigen receptor T (CAR-T) cell-induced CRS.9 Currently, randomized trails aiming to access the efficacy of tocilizumab in COVID-19 patients are still ongoing. What’s more, the timing of use of tocilizumab in relation to disease course also remains uncertain, it’s still unknown if earlier administration of this drug could prevent or decrease the progression of disease.10,11
To address this gap in the literature, we performed this meta-analysis on the available studies to date to investigate the efficacy and safety in COVID-19 patients. We also aim to provide evidence for the optimal timing for the administration of tocilizumab in peoples with COVID-19.
This meta-analysis was in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines.12 The protocol of the study was registered with the International Prospective Register of Systematic Reviews (PROSPERO) (ID: CRD42020191313).
Search strategy and selection criteria
Literature published in PubMed, EMBASE and Cochrane library databases were searched from the inception to June 23rd 2020, and no language restriction was placed in any databases. One epidemiologist was asked to look through all included studies and assess their eligibility for analysis. The following terms were used for the search: “COVID-19” or “coronavirus disease” or “novel coronavirus” or “SARS-CoV-2” and “tocilizumab”. Reference lists of eligible studies were manually searched for potentially eligible studies.
The inclusion criteria included studies that assessed the therapeutic efficacy of tocilizumab in patients with COVID-19. The inclusion criteria included: (Ⅰ) study population in each study were definitive diagnosis of coronavirus infection; (Ⅱ) studies that assessed the overall response rate (ORR) of tocilizumab in treatment of COVID-19 patients. We excluded all studies that could be classified as: (Ⅰ) the same cohorts enrolled in different studies; (Ⅱ) commentaries, editorials and case reports with a sample size less than 3 patients. In this study, we considered COVID-19 patients with severe disease experiencing acute respiratory distress syndrome (ARDS) and requiring mechanical ventilation or intensive care unit admission (ICU) support.
A total of 28 studies were finalized. Any disagreement between them was resolved by discussing with a third investigator. All studies were selected in two rounds, first on title and abstract and second on full text, according to the criteria mentioned above.
Data extraction and quality assessment
Two reviewers independently extracted relevant data from the selected studies in a standard form, a third reviewer assessed the extracted content, and a fourth investigator arbitrated on discrepancies between the first two reviewers. Any identified discrepancies were arbitrated by a fourth investigator.
We extracted the following variables: author, country, publication year, study design, sample size, comorbidity, treatment details (including timing, doses, route of tocilizumab, and other combined treatments), and ORR in the use of tocilizumab in severe and non-severe patients, mortality rate, length of ICU (LOI), length of hospitalization (LOH) and adverse reactions to tocilizumab. In this study, ORR was defined as the proportion of patients with clinical improvement after tocilizumab treatment, who were discharged or improved at least 2 points on the six-category ordinal scale during hospitalization: Ⅰ) being discharged from hospital with resumption of normal activities; Ⅱ) being discharged from hospital, but unable to resume normal activities; Ⅲ) hospitalization, not requiring supplemental oxygen; Ⅳ) hospitalization, requiring low-flow oxygen (FiO2<40%); Ⅴ) hospitalization requiring high-flow oxygen (FiO2≥40%), non-invasive mechanical ventilation, or both Ⅵ) hospitalization requiring extracorporeal membrane oxygenation (ECMO), invasive mechanical ventilation, or both Ⅶ) death.13 Patients with COVID-19 infection were categorized as having non-severe disease (outpatient care or admission to the general inpatient floor), or severe disease (mechanical ventilation or admission to ICU).
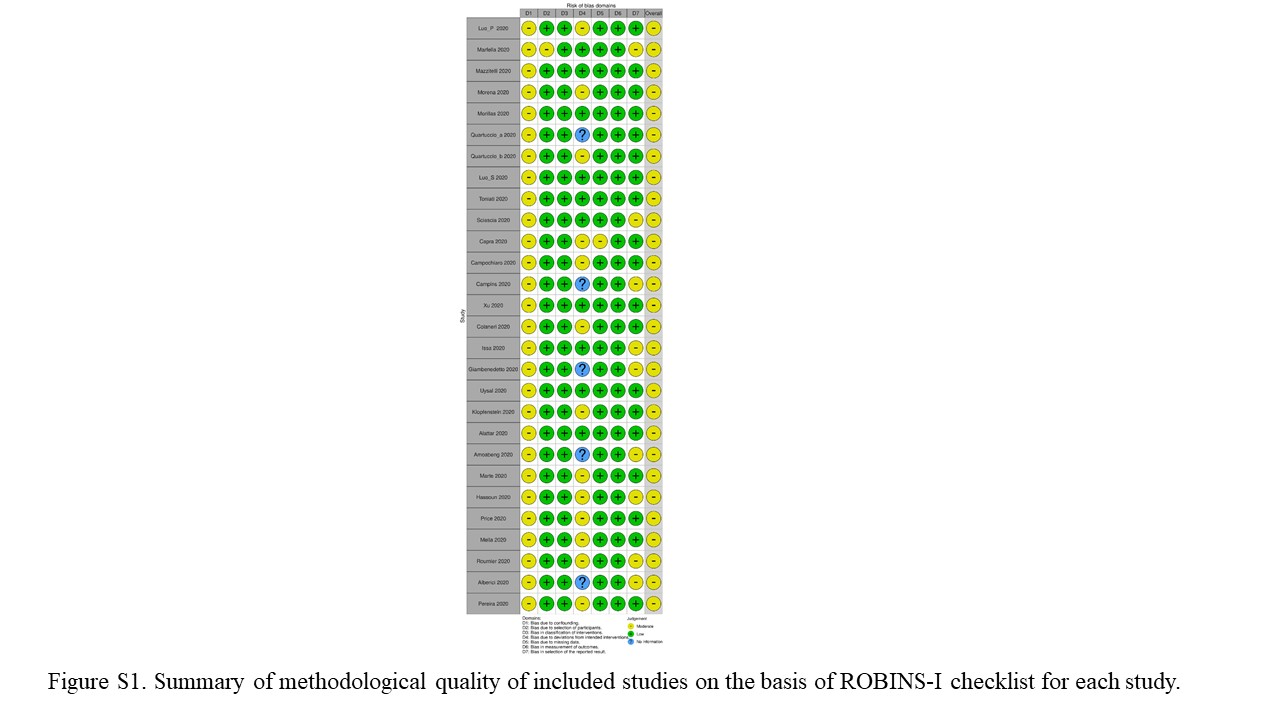
Quality assessment was done by two reviewers. We used ROBINS-I (Risk Of Bias In Non-randomized Studies-of Interventions) to evaluate the quality of original studies, which includes seven domains of bias due to confounding, bias in selection of participants into the study, bias in classification of interventions, bias due to deviations from intended interventions, bias due to missing data, bias in measurement of outcomes and bias in selection of the reported result. Eventually, an overall judgment on risk of bias for the outcome and result will be formulated on basis of all seven domains.14
Statistical analysis
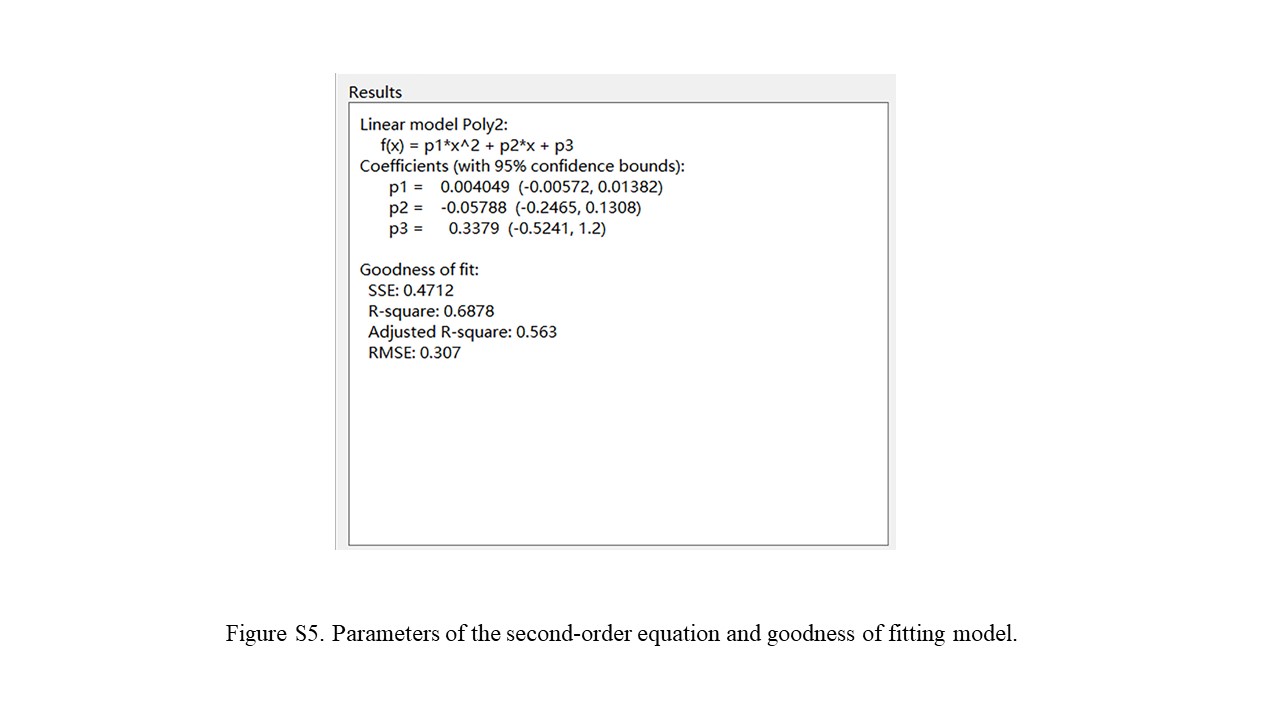
The primary outcome was to investigate the pooled ORR and mortality of tocilizumab in all COVID-19 patients, and in the severe and non-severe patients separately. The secondary outcome was the safety and optimal timing for administration of tocilizumab in COVID-19 patients. Risk ratio (RR) with 95% confidence intervals were calculated for dichotomized data, including ORR and mortality rate. Non-linear regression was applied to analyze the optimal timing from symptom onset to tocilizumab administration.15 Polynomial, logistic, and bell-shaped functions were used to fit all cause death-rate and mean time from symptom onset to tocilizumab administration. The second-order polynomial equation of a bell-shaped function was the following:

The adjusted coefficient of determination (R2) was selected to evaluate the goodness of the fitting models independently by the number of potential coefficients.16 If the original study only reports median and interquartile range, we used formulas to estimate the mean and standard deviation.17,18
Heterogeneity was assessed and using the inconsistency index (I2). Significant heterogeneity was defined as I2 >50% or P<0.05. To account for intra-study and inter-study variance, random-effects model was used for pooling all the ORR and mortality from separate study. Funnel plot was used to analyze potential publication bias. To evaluate the stability of results, sensitivity analysis was performed by repeating the analysis and omitting one article at a time.
R software version 3.6.2 (R Foundation for Statistical Computing), with the package meta was used for all statistical analyses and P<0.05 was considered statistically significant in this study.
A total of 279 unique publications was yielded in this study. According to flow diagram, 251 were excluded after primary and subsequent full-text review (Figure 1). Thus, 28 articles included 991 COVID-19 patients underwent tocilizumab administration were included in this study10,11,19-44. Of the 28 included studies, 7 of which included 377 patients were case-control studies with a control group not using tocilizumab28,29,32,36,39,40,42.
Baseline characteristics of all 28 included studies were listed in table 1. Of the total 991 patients, 769 were male (77.6%) and pooled median age was 62-year-old (range 55-73). The most common comorbidities were hypertension, cardiovascular disease and diabetes mellitus (DM). 324 patients undergone mechanical ventilation was reported in 19 studies. COVID-19 patients usually experience hyper-inflammation evidenced by exaggerated IL-6 and C-reactive protein (CRP). After administration of tocilizumab, most available data showed a dramatic drop of CRP value and serum IL-6 level tended to spike shortly in first and then decrease.
Quality assessment
Risk of bias of all studies was assessed by the ROBINS-I tool. Discriminations were primarily found in domain of “bias due to confounding” and “bias due to deviations from intended interventions”. Consequently, the overall judgment of risk of bias for all included studies was moderate (Figure S1).
Impact of tocilizumab treatment on ORR and mortality of COVID-19 patients
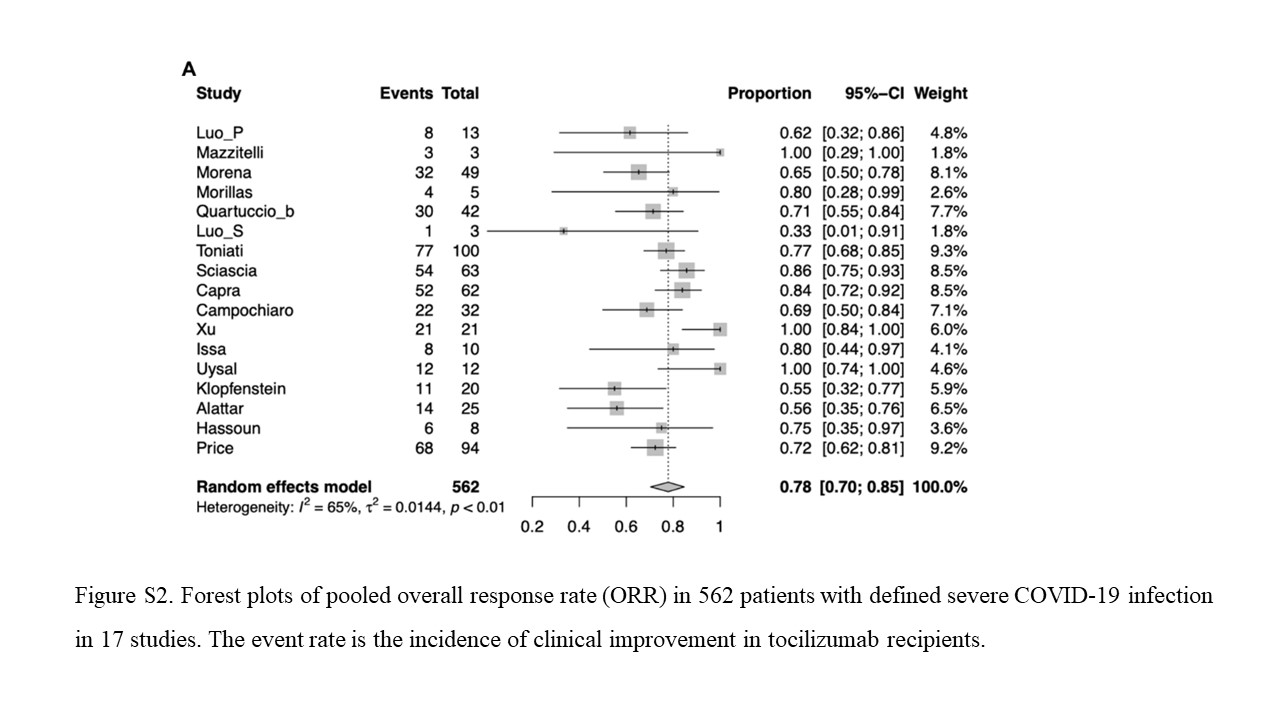
Of the 991 COVID-19 patients in all 28 studies, on top of antiviral treatment, additional use of tocilizumab was associated with a pooled ORR of 72% (95% CI, 66-79%; I2 = 72%, P< 0.0001) (Figure 2A). Data were unavailable for mortality in 3 studies, and a pooled all-cause death rate of 16% (95% CI, 11-22%; I2 = 67%, P< 0.0001) was reported in 870 patients when treated with tocilizumab. 17 studies10,11,19,21-23,25-29,31,33,35-37,40 comprising 562 patients were defined as severe COVID-19 infection, and the pooled ORR of treatment with tocilizumab was 78% (95% CI, 70-85%; I2 = 65%, P< 0.0001), while pooled ORR in 64 non-severe infection was 93% (95% CI, 85-98%; I2 = 0%, P=0.66) (Figure S2).
Of the 7 case-control studies, 377 patients had been assigned to tocilizumab therapy and 380 to standard-care treatment, the pooled results demonstrated a significantly lower risk of all-cause death at follow-up in patients with tocilizumab (RR: 0.61, 95% CI 0.42–0.90; P=0.012; Figure 3A). Moreover, Figure 3B illustrated that 231 patients received tocilizumab in experimental group also had a higher ORR than 269 patients in the control group, although the RR was statistically insignificance [1.10 (95% CI 0.96-1.27; P=0.175)].
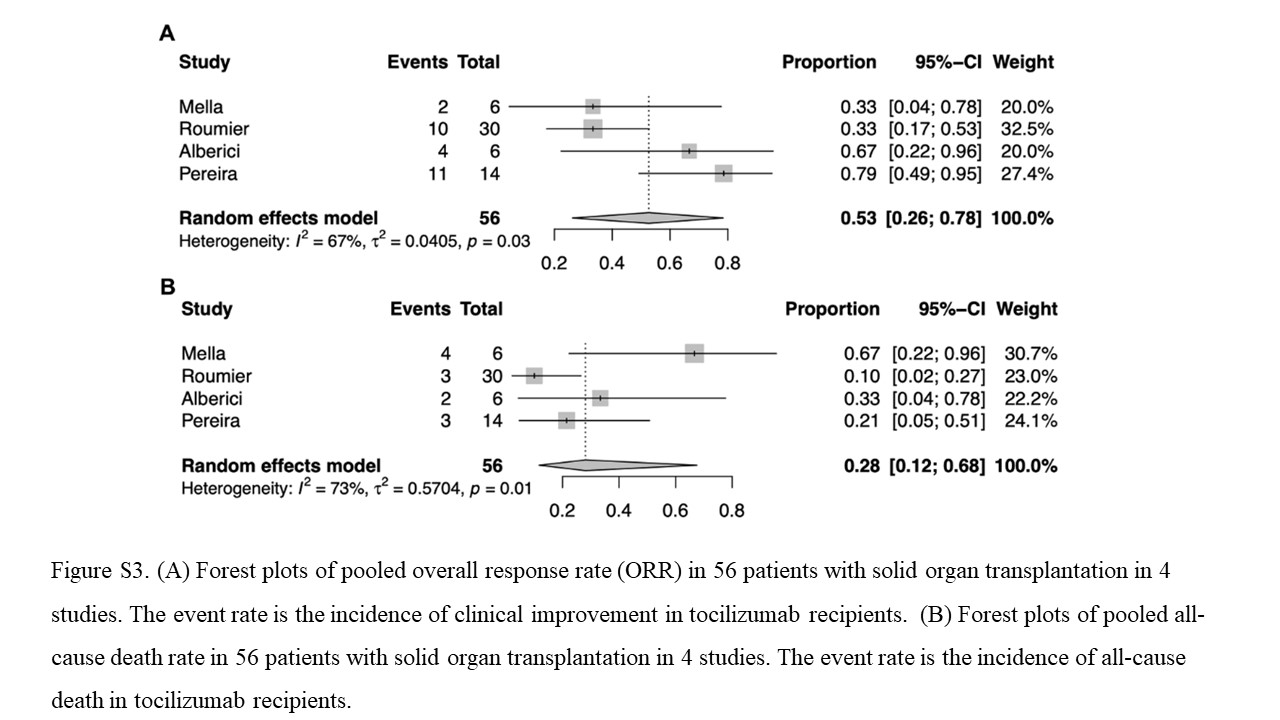
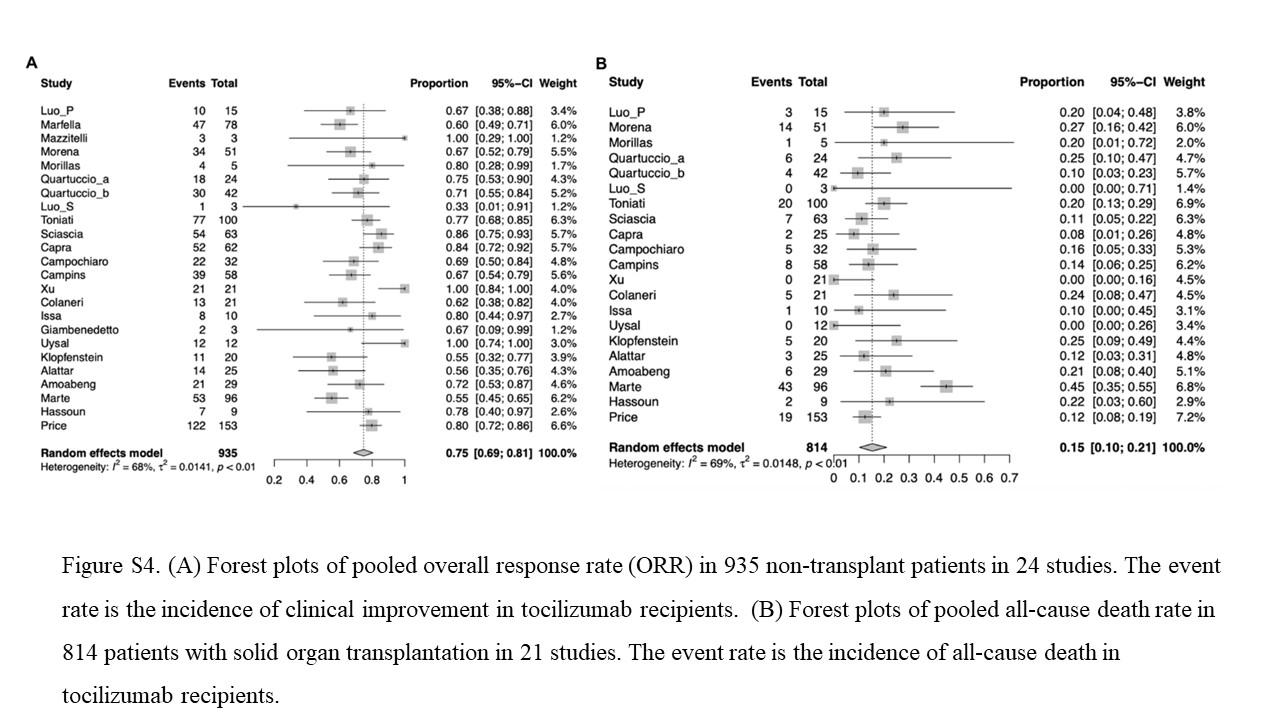
A subgroup analysis of 56 COVID-19 patients with solid organ transplantation indicated that the pooled ORR was 53% (95% CI, 26-78%; I2 = 67%, P=0.030) and the pooled all-death rate was 28% (95% CI, 12-68%; I2 = 73%, P=0.010) when compared with 935 non-transplant patients infected with COVID-19 (pooled ORR of 75%, 95% CI 69-81; I2 = 68%, P< 0.0001 and pooled all-death rate of 15%, 95% CI 10-21%; I2 = 69%, P< 0.0001). Overall, these results presented a poorer clinical outcome in solid organ transplant recipients than non-transplant patients when administrated tocilizumab (Figure S3 and S4).
Impact of tocilizumab treatment on duration of hospitalization, ICU stay and mechanical ventilation
At the point of study completion, median LOH and LOI was 14 days (range 11-34) and 8 days (range 5-11) in patients receiving tocilizumab, which was specified in 15 studies10,20-23,28,29,31,32,35,36,38-41 and 8 studies10,23,27,29,32,33,36,42 , separately. Moreover, the median duration of mechanical ventilation was 7 days (range 5-10) after treatment of tocilizumab which was documented in 9 articles10,11,21-23,27,28,40,41 (Table 2).
Optimal timing and safety in use of tocilizumab
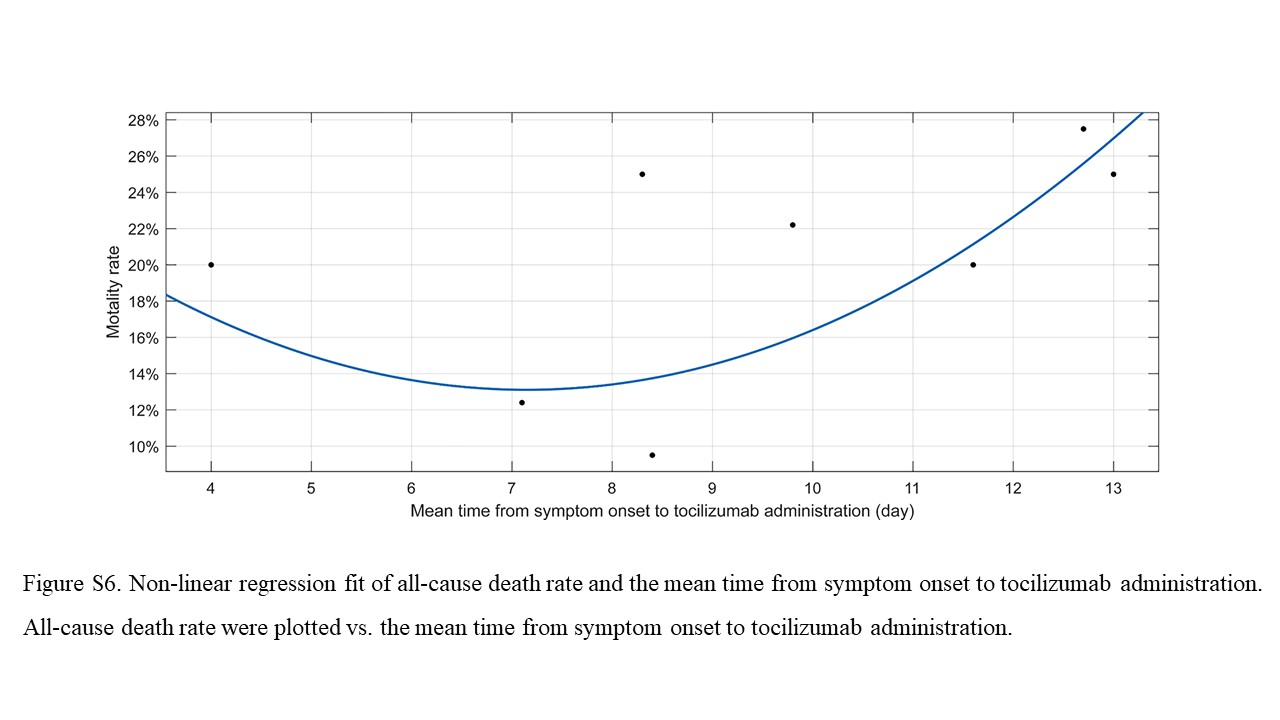
The timing of tocilizumab administration was clarified in 8 studies.10,22-25,27,36,40 With this data, the second-order polynomial equation was given as following: y = p1*x2 + p2*x + p3. (p1 = 0.004099 (-0.006127, 0.01433), p2 = -0.05933 (-0.257, 0.1384), p3 = 0.3474 (-0.5564, 1.251). The significance of the model was inferred by P value (P<0.001), and the goodness of fit was accessed by R2 which was 0.667 (Figure S5). Thus, we deduced, by this polynomial equation, that the optimal timing of tocilizumab administration was the 7.15 day from the symptom onset and with a lowest all-cause death rate of 13.11% (Figure S6).
Nearly all included studies confirmed the safety of tocilizumab for treatment of COVID-19 patients no matter in the context of ICU or general ward. Although the occurrence was very low, the most commonly reported adverse events were the elevation of hepatic enzymes of at least 3-times above the normal level, pancytopenia and cutaneous rash. (Table 3) Occasionally, bacteremia caused by neutropenia was reported by individual medical centers.
Publication bias and sensitivity analysis
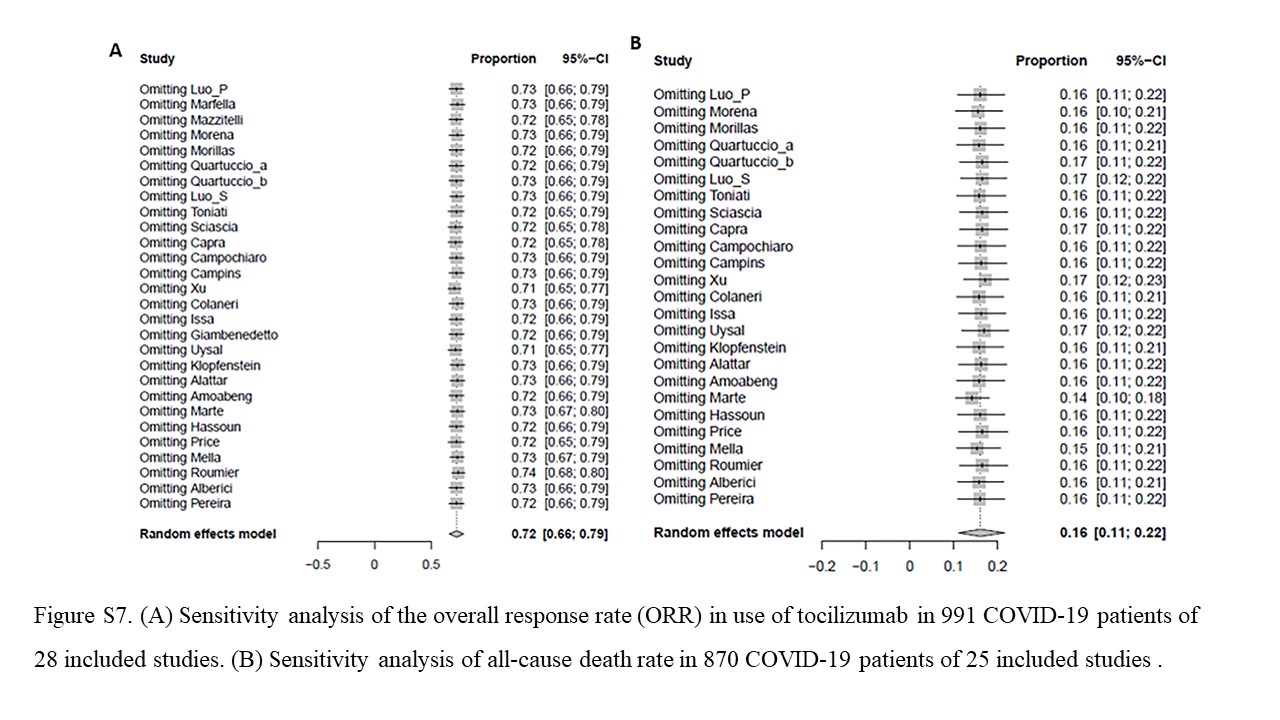
The funnel plots were used to assess the evidence of bias towards studies. According to the Figure 4, there was no conclusive evidence of publication bias of ORR and mortality in any studies (P=0.611 and P=0.875). In the sensitivity analysis, the overall estimates remained consistent across the analysis of ORR and all-cause death rate in all included studies, which suggests our results were credible. (Figure S7)
To the best of our knowledge, this is the first study to investigate the efficacy and safety of COVID-19 patients who were treated with tocilizumab. Our study is also the first meta-analysis to evaluate the optimal timing of tocilizumab administration. The result of this study showed that the tocilizumab seems to be an effective and safe treatment of COVID-19 patients. While the therapeutic role for tocilizumab can be considered, regardless of the concomitant antiviral agents, our finding was also confirmed in case-control study. Moreover, we also identified the optimal time of tocilizumab administration which was helpful to reduce the rate of mortality.
The pandemic of COVID-19 has confronted global health with unprecedent threat. However, since SARS-CoV-2 is a newly emerging virus, an absolute consensus on such a controversial issue has not been reached at present. According to a large report, all-cause mortality rate of 2087 critically-ill patients with COVID-19 was an astonishing 49%.45 Other studies from different centers found the mortality rates of 62% (in Wuhan, China) and 67% (in Washington State, USA) of all patients in the ICU.46,47 Moreover, previous study also reported that the median duration of ICU stay was 10.6 days of 1840 COVID-19 patients from California and Washington.48 Over 50% of patients were with a length of hospital stay of 20 days or more.49
Immunomodulatory agents remain a promising strategy for the treatment of severe COVID-19, since it can attenuate the increased inflammatory response of the patients. Therefore, tocilizumab was considered as a promising therapeutic option to COVID-19 patients. Analysis of all studies indicated a clear clinical improvement in 78% identified critically ill cases and the all-cause death rate is 16% in all patients. Moreover, duration of hospitalization and ICU stay may also decline after concomitant use of tocilizumab. Thus, pooled results of included studies from different medical centers support the concept that tocilizumab treatment may improve the clinical outcome of COVID patients.
The optimal treatment of immunosuppression in COVID-19 patients underwent solid organ transplantation remains uncertain despite the urgency and importance of this issue. Pereira et al. reported that 14 patients have received 1-3 doses of tocilizumab with no adverse events noted, however, transplant recipients may be at high risk of severe disease of COVID-19 and poor outcomes.44 The results of this study also confirmed that lower ORR and higher all-cause death rate was documented in these patients after tocilizumab therapy. There is still an urgent need to identify the most effective treatment strategies in this cohort.
Generally, the route and dose of tocilizumab administration was based on previously studies of pharmacokinetic and pharmacodynamics analysis50, with the dose of 8mg/kg (or 400mg per dose) i.v. or s.c., a second dose of 400 mg of tocilizumab may also be utilized due to deterioration of the disease. Thus, the results of optimal dose were still heterogeneous and may be based on drug availability in each center. Importantly, on basis of mathematical models and parameters, we inferred that 7.15 day from the symptom onset to tocilizumab administration appeared to the optimal time point to minimize the mortality of COVID-19 patients.
Safety profile of tocilizumab is another big concern when utilized in COVID-19 patients. Our analysis showed that some individuals receiving tocilizumab may experience adverse reactions which often involve elevation of hepatic enzymes, pancytopenia and cutaneous rash. According to a previous study, the main concern regarding tocilizumab administration is the occurrence of severe bacterial infection.51 However, only very few studies have reported data on severe infection in patients underwent tocilizumab, and it was definitely not a contraindication for tocilizumab administration, particularly in critical patients.
There are some limitations in this study. Firstly, the efficacy of tocilizumab may be influenced by other agents, such as various antiviral treatment and (or) hydroxychloroquin. In view of this, we conducted a subgroup analysis in all case-control studies, and nearly a third of all 991 patients have the controls who underwent a same therapeutic strategy without tocilizumab. Similar results were found when the subgroup was analyzed, and with a lower all-cause death rate and higher ORR in the tocilizumab group. Secondly, there is no uniform standard for the time and dosage of tocilizumab used in various studies. But, perhaps for that reason, an optimal time of application was actually needed more than ever. Thirdly, some data of laboratory and radiological findings were not available in most of studies. Meta-regression cannot be performed to investigate the potential risk factors of prognosis for COVID-19 patients on tocilizumab treatment. Finally, due to the rapid evolution of the management of COVID-19, results of some ongoing randomized controlled clinical trials cannot be reached which will lead to publication bias.
Administration of tocilizumab in subjects with COVID-19 infection, seemingly improve clinical outcome and alleviate the duration of hospitalization or ICU stay. The occurrence of adverse events was low, nearly all studies confirmed the safety of tocilizumab administration. Thus, the use of tocilizumab seems to be beneficial in some of the COVID-19 patients to suppress the immune response, especially in severe cases. The optimal timing of tocilizumab administration, if confirmed, is likely to provide the guidance for management of COVID-19 patients.
However, tocilizumab should be used with caution in solid transplant recipients for its suboptimal performance. Prospective data on clinical outcomes from randomized trials are warranted to further verify this conclusion.
Funding
None
Competing interests
None
- Guan, W. J. et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med 382, 1708-1720 (2020).
- Yu, N. et al. Clinical features and obstetric and neonatal outcomes of pregnant patients with COVID-19 in Wuhan, China: a retrospective, single-centre, descriptive study. Lancet Infect Dis 20, 559-564 (2020).
- Mehta, P., McAuley, D. F., Brown, M., Sanchez, E., Tattersall, R. S. & Manson, J. J. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet 395, 1033-1034 (2020).
- Shimabukuro-Vornhagen, A. et al. Cytokine release syndrome. J Immunother Cancer 6, 56 (2018).
- Zhu, J., Pang, J., Ji, P., Zhong, Z., Li, H., Li, B. & Zhang, J. Elevated interleukin-6 is associated with severity of COVID-19: a meta-analysis. J Med Virol (2020).
- Zhou, F. et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 395, 1054-1062 (2020).
- Ruan, Q., Yang, K., Wang, W., Jiang, L. & Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med 46, 846-848 (2020).
- Schoels, M. M. et al. Blocking the effects of interleukin-6 in rheumatoid arthritis and other inflammatory rheumatic diseases: systematic literature review and meta-analysis informing a consensus statement. Ann Rheum Dis 72, 583-589 (2013).
- Le, R. Q. et al. FDA Approval Summary: Tocilizumab for Treatment of Chimeric Antigen Receptor T Cell-Induced Severe or Life-Threatening Cytokine Release Syndrome. Oncologist 23, 943-947 (2018).
- Hassoun, A., Thottacherry, E. D., Muklewicz, J., Aziz, Q. U. & Edwards, J. Utilizing tocilizumab for the treatment of cytokine release syndrome in COVID-19. J Clin Virol 128, 104443 (2020).
- Sciascia, S. et al. Pilot prospective open, single-arm multicentre study on off-label use of tocilizumab in patients with severe COVID-19. Clin Exp Rheumatol 38, 529-532 (2020).
- Moher, D., Liberati, A., Tetzlaff, J. & Altman, D. G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6, e1000097 (2009).
- Cao, B. et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19. N Engl J Med 382, 1787-1799 (2020).
- Sterne, J. A. et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355, i4919 (2016).
- Kalathinathan, P. & Kodiveri, M. G. A statistical approach for enhanced production of β-galactosidase from Paracoccus sp. and synthesis of galacto-oligosaccharides. Folia Microbiol (Praha) (2020).
- Iosa, M., Paolucci, S. & Morone, G. Covid-19: A Dynamic Analysis of Fatality Risk in Italy. Front Med (Lausanne) 7, 185 (2020).
- Shi, J., Luo, D., Weng, H., Zeng, X. T., Lin, L., Chu, H. & Tong, T. Optimally estimating the sample standard deviation from the five-number summary. Res Synth Methods (2020).
- Luo, D., Wan, X., Liu, J. & Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res 27, 1785-1805 (2018).
- Luo, P., Liu, Y., Qiu, L., Liu, X., Liu, D. & Li, J. Tocilizumab treatment in COVID-19: A single center experience. J Med Virol 92, 814-818 (2020).
- Marfella, R. et al. Negative impact of hyperglycaemia on tocilizumab therapy in Covid-19 patients. Diabetes Metab (2020).
- Mazzitelli, M. et al. Use of subcutaneous tocilizumab in patients with COVID-19 pneumonia. J Med Virol (2020).
- Morena, V. et al. Off-label use of tocilizumab for the treatment of SARS-CoV-2 pneumonia in Milan, Italy. Eur J Intern Med 76, 36-42 (2020).
- Morillas, J. A. et al. Tocilizumab therapy in five solid and composite tissue transplant recipients with early ARDS due to SARS-CoV-2. Am J Transplant (2020).
- Quartuccio, L., Sonaglia, A., Pecori, D., Peghin, M., Fabris, M., Tascini, C. & De Vita S. Higher levels of IL-6 early after tocilizumab distinguish survivors from non-survivors in COVID-19 pneumonia: a possible indication for deeper targeting IL-6. J Med Virol (2020).
- Quartuccio, L. et al. Profiling COVID-19 pneumonia progressing into the cytokine storm syndrome: Results from a single Italian Centre study on tocilizumab versus standard of care. J Clin Virol 129, 104444 (2020).
- Luo, S., Yang, L., Wang, C., Liu, C. & Li, D. [Clinical observation of 6 severe COVID-19 patients treated with plasma exchange or tocilizumab]. Zhejiang Da Xue Xue Bao Yi Xue Ban 49, 227-231 (2020).
- Toniati, P. et al. Tocilizumab for the treatment of severe COVID-19 pneumonia with hyperinflammatory syndrome and acute respiratory failure: A single center study of 100 patients in Brescia, Italy. Autoimmun Rev 19, 102568 (2020).
- Capra, R., De Rossi N, Mattioli, F., Romanelli, G., Scarpazza, C., Sormani, M. P. & Cossi, S. Impact of low dose tocilizumab on mortality rate in patients with COVID-19 related pneumonia. Eur J Intern Med 76, 31-35 (2020).
- Campochiaro, C. et al. Efficacy and safety of tocilizumab in severe COVID-19 patients: a single-centre retrospective cohort study. Eur J Intern Med 76, 43-49 (2020).
- Campins, L., Boixeda, R., Perez-Cordon, L., Aranega, R., Lopera, C. & Force, L. Early tocilizumab treatment could improve survival among COVID-19 patients. Clin Exp Rheumatol 38, 578 (2020).
- Xu, X. et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc Natl Acad Sci U S A 117, 10970-10975 (2020).
- Colaneri, M. et al. Tocilizumab for Treatment of Severe COVID-19 Patients: Preliminary Results from SMAtteo COvid19 REgistry (SMACORE). Microorganisms 8, (2020).
- Issa, N., Dumery, M., Guisset, O., Mourissoux, G., Bonnet, F. & Camou, F. Feasibility of Tocilizumab in ICU patients with COVID-19. J Med Virol (2020).
- Di, G. S. et al. Off-label Use of Tocilizumab in Patients with SARS-CoV-2 Infection. J Med Virol (2020).
- Borku, U. B. et al. ''Tociluzumab challenge: A series of cytokine storm therapy experience in hospitalized Covid-19 pneumonia patients''. J Med Virol (2020).
- Klopfenstein, T. et al. Tocilizumab therapy reduced intensive care unit admissions and/or mortality in COVID-19 patients. Med Mal Infect (2020).
- Alattar, R. et al. Tocilizumab for the treatment of severe coronavirus disease 2019. J Med Virol (2020).
- Antwi-Amoabeng, D., Kanji, Z., Ford, B., Beutler, B. D., Riddle, M. S. & Siddiqui, F. Clinical outcomes in COVID-19 patients treated with tocilizumab: An individual patient data systematic review. J Med Virol (2020).
- Rojas-Marte, G. R. et al. Outcomes in Patients with Severe COVID-19 Disease Treated with Tocilizumab - A Case- Controlled Study. QJM (2020).
- Price, C. C. et al. Tocilizumab treatment for Cytokine Release Syndrome in hospitalized COVID-19 patients: survival and clinical outcomes. Chest (2020).
- Mella, A. et al. Case series of six kidney transplanted patients with COVID-19 pneumonia treated with tocilizumab. Transpl Infect Dis e13348 (2020).
- Chaidos, A., Katsarou, A., Mustafa, C., Milojkovic, D. & Karadimitris, A. Interleukin 6-blockade treatment for severe COVID-19 in two patients with multiple myeloma. Br J Haematol (2020).
- Alberici, F. et al. [Managing patients in dialysis and with kidney transplant infected with Covid-19]. G Ital Nefrol 37, (2020).
- Pereira, M. R. et al. COVID-19 in solid organ transplant recipients: Initial report from the US epicenter. Am J Transplant (2020).
- Wu, Z. & McGoogan, J. M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA (2020).
- Yang, X. et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 8, 475-481 (2020).
- Arentz, M., Yim, E., Klaff, L., Lokhandwala, S., Riedo, F. X., Chong, M. & Lee, M. Characteristics and Outcomes of 21 Critically Ill Patients With COVID-19 in Washington State. JAMA (2020).
- Lewnard, J. A. et al. Incidence, clinical outcomes, and transmission dynamics of severe coronavirus disease 2019 in California and Washington: prospective cohort study. BMJ 369, m1923 (2020).
- Ye, C. et al. Clinical features of rheumatic patients infected with COVID-19 in Wuhan, China. Ann Rheum Dis (2020).
- Morcos, P. N., Zhang, X., McIntyre, C., Bittner, B., Rowell, L. & Hussain, Z. Pharmacokinetics and pharmacodynamics of single subcutaneous doses of tocilizumab administered with or without rHuPH20. Int J Clin Pharmacol Ther 51, 537-548 (2013).
- Pawar, A. et al. Risk of serious infections in tocilizumab versus other biologic drugs in patients with rheumatoid arthritis: a multidatabase cohort study. Ann Rheum Dis 78, 456-464 (2019).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}