Glioblastoma (GB) metastasis beyond the central nervous system (CNS) is exceptionally rare, mainly due to the protective function of the blood-brain barrier (BBB), the lack of lymphatic drainage, and the typically short overall survival (OS) of this aggressive malignancy 10. Previous studies have reported that the average interval from initial diagnosis to extracranial tumor dissemination is around 11 months 11, 12. Metastasis to vertebral sites, however, tends to occur later, with a median time of around 26 months 11, 12.
The mechanisms behind GB metastasis outside the CNS remain unclear, but are believed to involve a mix of iatrogenic, genetic, and molecular factors, requiring further research 10. Identified risk factors for extracranial metastasis include craniotomy, stereotactic biopsy, ventricular shunting, younger age, radiation therapy, prolonged survival, tumor recurrence, and sarcomatous components 10. Over 90% of patients with extracranial metastases have had craniotomy, suggesting that glial cell dissemination through the bloodstream during surgery is a likely pathway for spread 13, 14.
GB cells may also metastasize via cerebrospinal fluid through peritoneal shunts or by seeding soft tissues through craniotomy defects. Chronic wound infections and tumor resection may increase the risk of extracranial metastasis due to direct surgical seeding 15, 16. The mechanisms driving the osteolytic metastasis of GB are hypothesized to involve complex, bidirectional interactions between brain tumor cells and bone tissue 17.
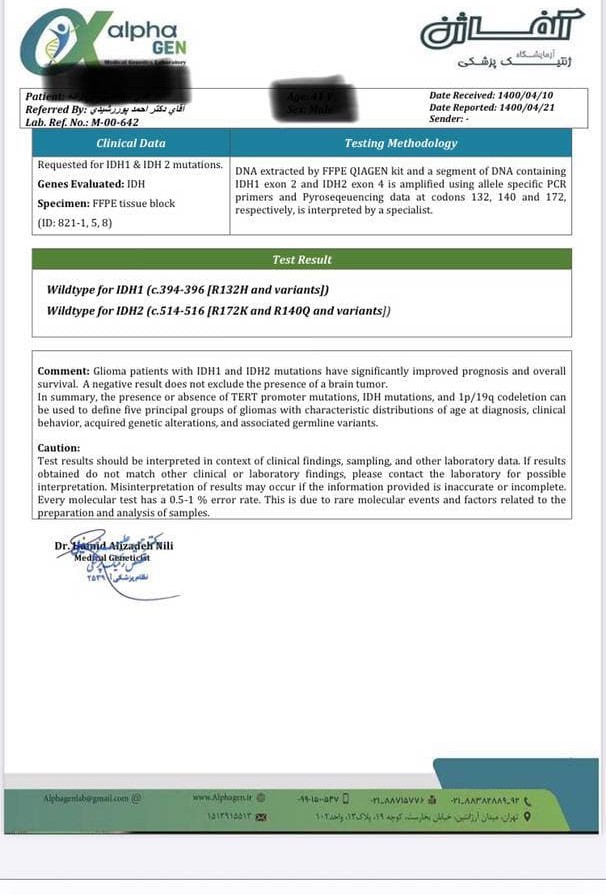
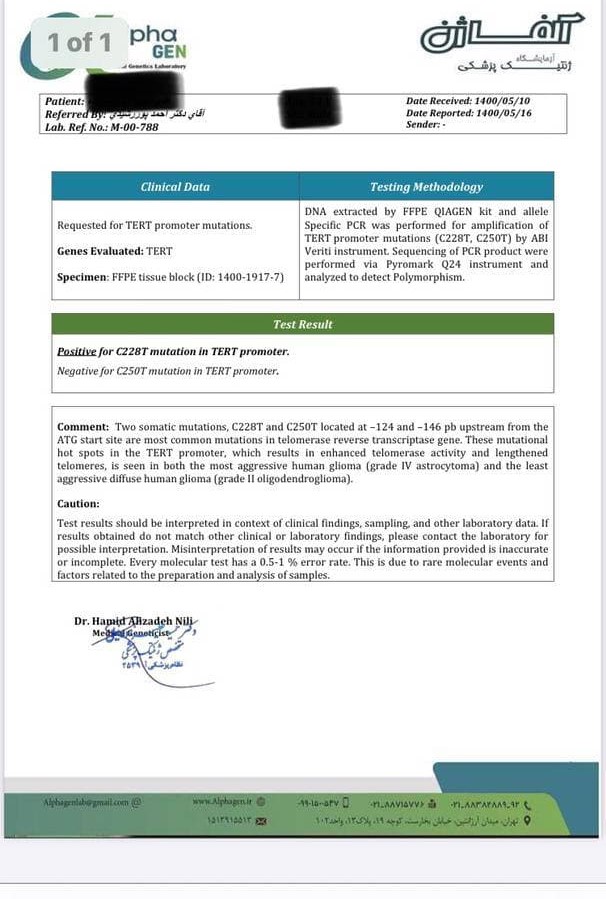
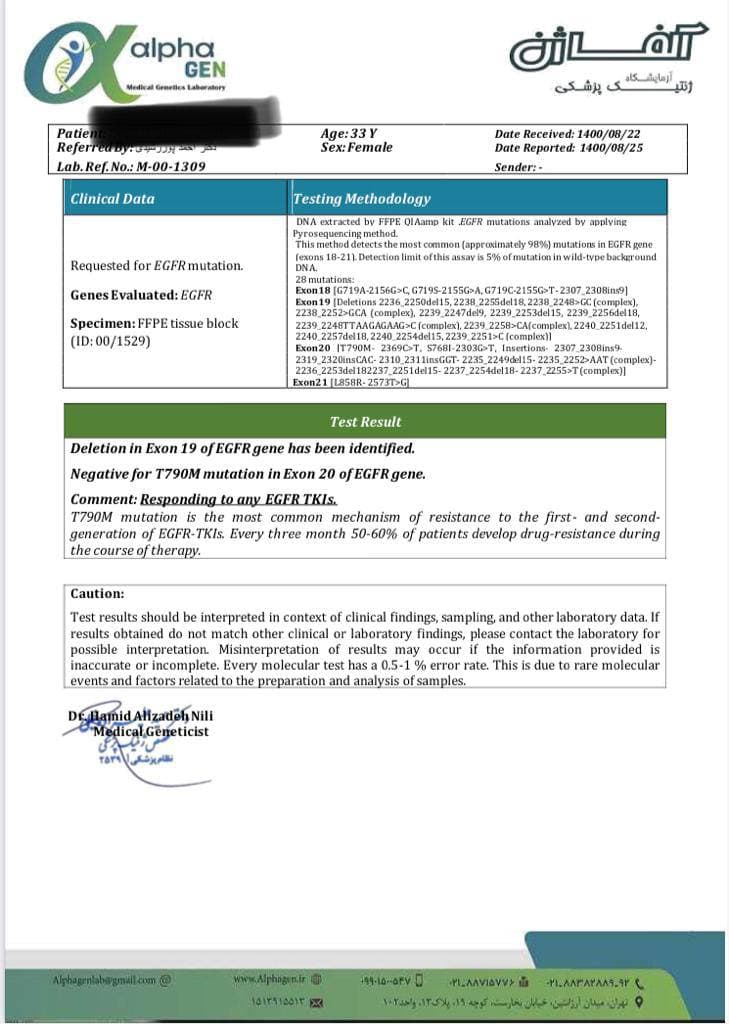
Despite extensive research on molecular variants associated with glioblastoma (GB) and its subtypes, a critical gap persists in identifying genomic drivers enabling GB metastasis. Through protein-protein interaction network reconstruction, we identified six key genes—Ubiquitin C (UBC), Fibronectin 1 (FN1), Epidermal Growth Factor Receptor (EGFR), Catenin Beta 1 (CTNNB1), Jun Proto-Oncogene (JUN), and Mitogen-Activated Protein Kinase 1 (MAPK1)—that may play pivotal roles in GB invasion
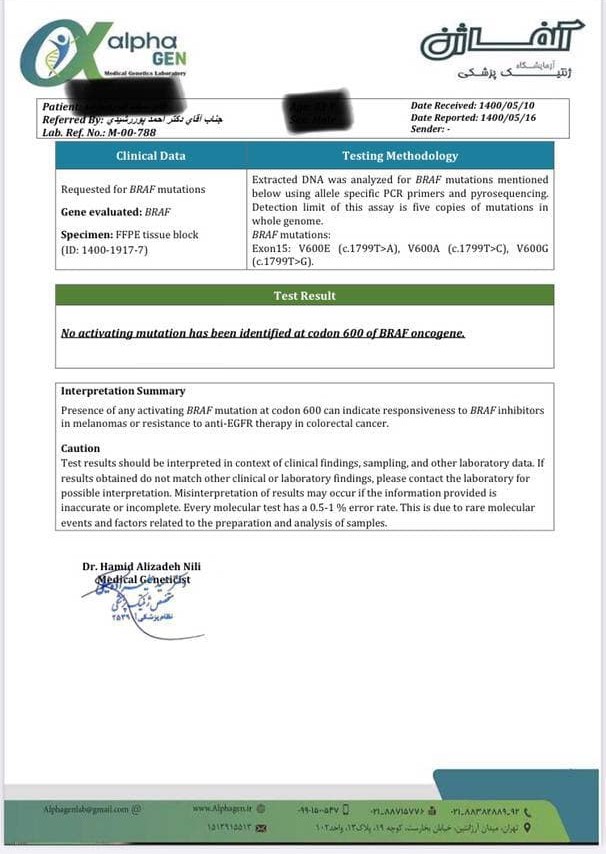
FN1, in particular, has been suggested as a diagnostic marker to differentiate GB from low-grade astrocytoma, with its expression playing a functional role in the progression of malignant gliomas through the TGF-β-induced epithelial-mesenchymal transition (EMT) pathway 18. Hendrych et al. identified genetic alterations in NF1, NOTCH3, AIRDA1, and MTOR in cases of glioblastoma metastasizing to the spine. Interestingly, while the BRAF mutation is commonly found in primary tumors, it is absent in metastatic lesions, where NF1 mutations are detected, indicating that tumor cells lacking the BRAF mutation may acquire metastatic potential 19. Moreover, the Epidermal Growth Factor (EGF) has been shown to promote glioblastoma metastasis by inducing matrix metalloproteinase-9 (MMP-9) through an EGFR-dependent mechanism 20. In the context of metastasis, the aberrant activation of MAPK signaling in glioblastoma cells is believed to enhance their invasive capacity, potentially leading to the formation of secondary tumors at distant sites, although extracranial metastasis remains a rare occurrence 21, 22.
In recurrent GB, metabolism shifts toward increased glycolysis, altered lipid and amino acid metabolism, and enhanced hypoxia-driven pathways. Metastatic GB adapts further, utilizing diverse energy sources, boosting antioxidant defenses, and remodeling the extracellular matrix, demonstrating distinct metabolic strategies at each stage. 23. In other words, transitioning from recurrence to metastasis is a journey from mere survival to profound adaptation
Our results revealed that phenylalanine, tyrosine, and arginine pathways were unique to the recurrent DBS samples, while aspartate and glutamate were exclusive to metastasis DBS. Notably, many tumours rely on arginine, as they lack the ability to synthesize it. 24, 25. Arginine deprivation causes elongated cell morphology and loss of intracellular lamellipodia, inhibiting cell motility, adhesion, and invasion. In GB, arginylation is crucial for actin assembly, and arginine deprivation reduces N-terminal arginylation of β-actin, impairing these processes 26.
Glutamine is the most depleted amino acid in tumor cells. It serves as a crucial metabolic fuel, meeting the extensive energy demands of metastatic cells for ATP, biosynthetic precursors, and reductants 23. Enhanced glutamine availability bolsters cancer cell invasiveness, facilitating distant metastasis. Brain metastatic tumor cells, exhibiting metabolic plasticity, can derive energy from non-glucose sources, notably utilizing glutamine and branched-chain amino acids (BCAAs) as alternative fuels 27, 28. Brain metastases show a significant reliance on glutamine metabolism, with overexpression of xCT promoting cystine uptake and glutamine oxidation, thus aiding metabolic adaptation and redox balance 29. Given the brain's high demand for glutamate, cells require an amino group donor, primarily sourced from BCAAs, to sustain glutamate anabolism. Consequently, cerebral vascular endothelial cells express numerous neutral amino acid transporters to support substantial BCAA uptake 30, 31. Additionally, aspartate metabolism has been linked to tumor metastasis, where metastatic cancer cells consume substantial glutamine to compensate for TCA cycle deficiencies, increasing their dependence on asparagine. Inhibiting asparagine synthetase (ASNS) can induce rapid apoptosis in these metastatic cells 32.
Serine and glycine are critical amino acids required substantially during metastasis to support biosynthetic processes such as glycolysis, glutathione synthesis, and nucleotide production 33. In the microenvironment of brain metastases, the levels of serine and glycine are notably lower than in plasma 34, likely due to the high demand of metastatic tissues for these amino acids 35. Tryptophan metabolism is also crucial in glioblastoma progression, exhibiting distinct alterations between recurrent and metastatic stages. In recurrent GB, Indoleamine 2,3-dioxygenase (IDO) upregulation shifts tryptophan metabolism toward kynurenine production, activating the hydrocarbon receptor (AhR) pathway to enhance immune suppression and treatment resistance. During metastasis, the kynurenine pathway demonstrates metabolic flexibility, adapting tryptophan degradation to different microenvironments, thereby further promoting immune evasion, tumor invasion, and colonization 36, 37.
In summary, GB) metastasis beyond the central nervous system (CNS) remains exceptionally rare due to the protective BBB and the typically short overall survival. However, when it occurs, it is often facilitated by iatrogenic factors and complex molecular mechanisms. Our study underscores the critical role of metabolic adaptations in GB progression, highlighting how recurrent tumors rely on altered metabolic pathways for survival while metastatic cells exploit diverse energy sources and display metabolic plasticity. Notably, the significant depletion of specific amino acids and the adaptation of tryptophan metabolism reveal potential therapeutic targets. Despite these insights, understanding the complete mechanisms of GB metastasis remains challenging, necessitating further research into the genomic drivers and metabolic dependencies of this aggressive malignancy.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}