Demographics and Training
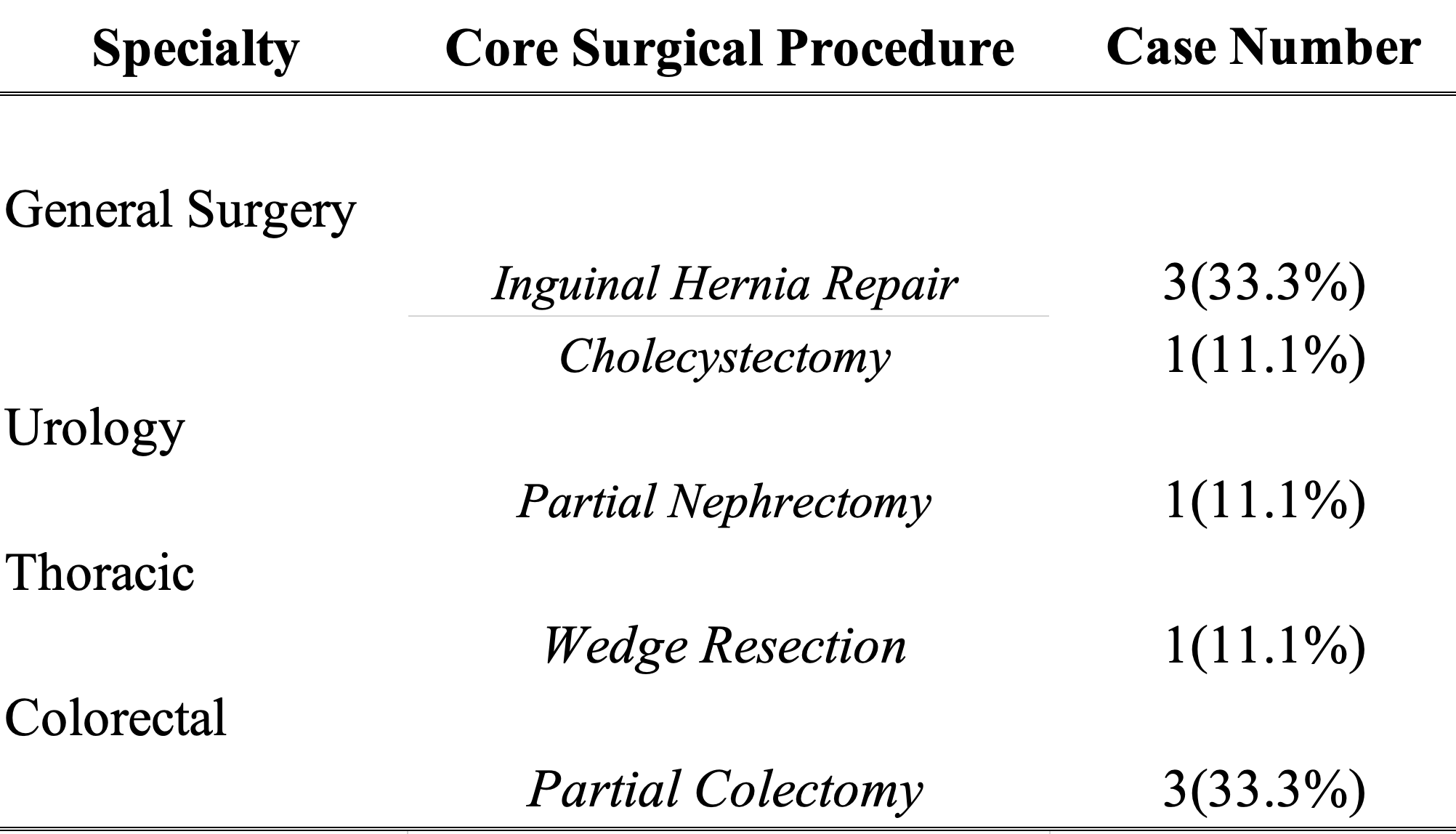
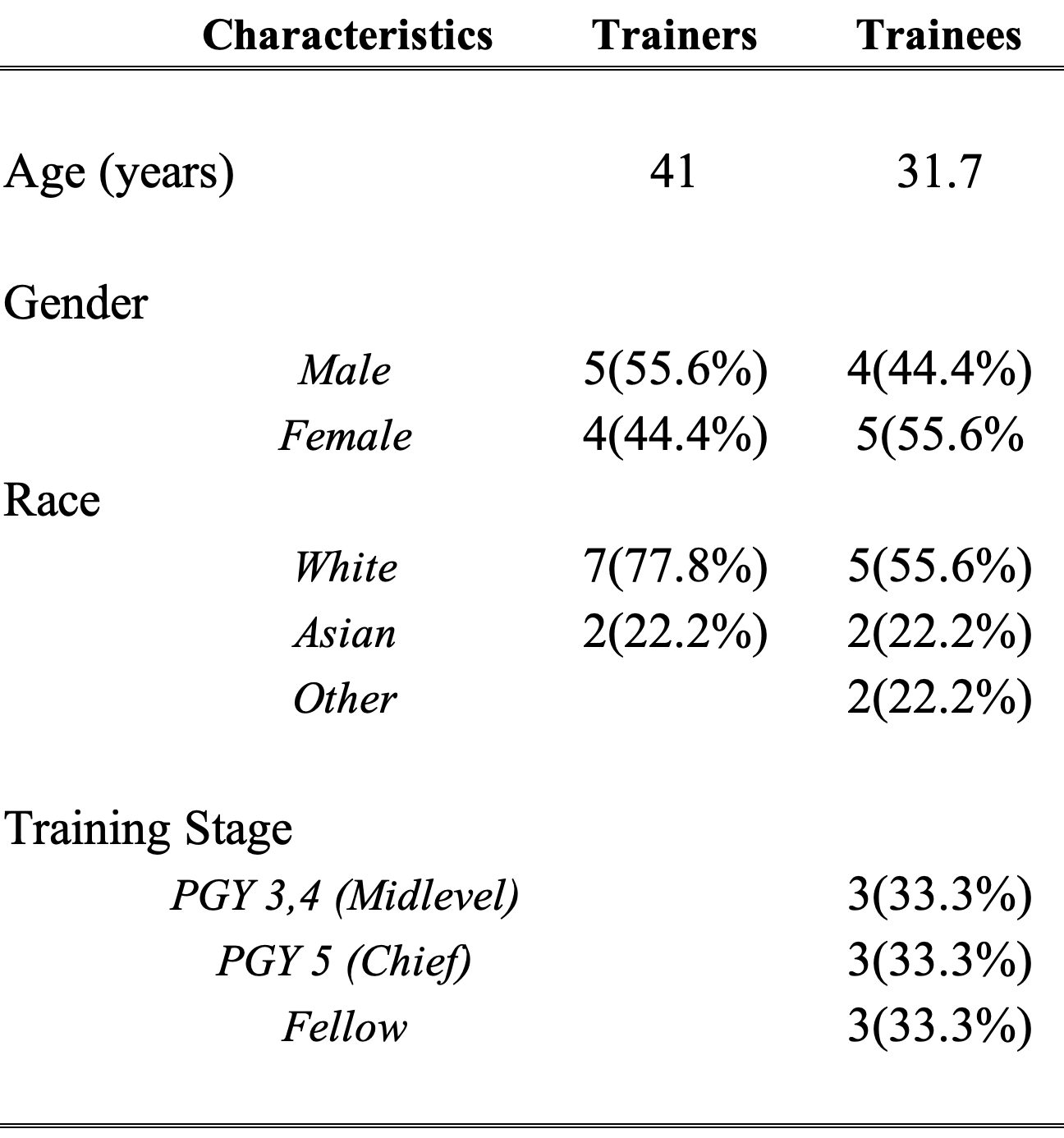
A total of nine robotic surgery procedures between May and September 2023 were included. Of the 9 procedures, 4 were Colorectal, 3 General Surgery, 1 Thoracic Surgery, and 1 Urology. (Table 1) 9 trainers and 9 trainees participated and completed surveys. Demographic information is summarized in Table 2. The 9 trainees had an average age of 31.7 years. 44.4% of the trainees identified as men and 55.6% identified as women. 55.6% trainees identified as white, 22.2% as Asian and 22.2% as others. 33.3% of trainees were mid-level residents (PGY3, 4), 33.3% were chief residents (PGY5), and 33.3% were first year fellows. The 9 trainers had an average age of 41 years. 55.6% identified as men and 44.4% identified as women. 77.8% identified as white and 22.2% identified as Asian. The range of combined training and practice was between 11- 25 years.
Quantitative Analysis
The average overall trainee console time was 47.3% ± 16.2, with a range between 31.4% and 74.3%, and notable differences between mid-level residents 49.1%±14.8, chiefs 38.5%± 21.1, and fellows 54.2%± 13.8. The average overall trainer console time was 52.7% ± 16.2 with a range between 25.7% and 68.6%. The average trainee mLMX trust score was 3.83±0.66 with a range between 2.88 and 4.77. The average trainer mLMX trust score was 3.67±0.71 with a range between 2.77 and 4.77.
Correlation analysis between the average trainer mLMX trust score and trainee console time yielded a Pearson coefficient of r=0.547 (Figure 2A). Similarly, correlation between the average trainee mLMX trust score and trainee console time yielded a Pearson correlation coefficient of r=-0.19 (Figure 2B). Additionally, correlation analysis between the average trainer mLMX trust score and average trainee mLMX trust scores yielded a Pearson correlation coefficient of r=0.329 (Figure 2C).
Trainees were then stratified into 2 groups based on their console times; >50% and <50%. 55.6% of trainees had a console time >50% and 44.4% had a console time <50%. Average trainer mLMX trust score was 4.08 for trainees with >50% console time as opposed to 3.16 for trainees with < 50% console time (p=0.038*). Moreover, average trainee mLMX trust score was 3.92 for trainees with >50% console time as opposed to 3.76 for trainees with < 50% console time (p=0.74).
Qualitative Analysis
Thematic analysis revealed a robust educational environment. Despite the use of isolated consoles, there was evidence of dynamic interaction and didactic exchange between trainers and trainees. Three major themes from our qualitative review demonstrated clear interactions between trust-autonomy and training dynamics (teaching, feedback, and communication) in the robotic surgery operating room: 1) effective teaching techniques, 2) feedback escalation, and 3) trust fostering behaviors. (Figure 3)
Effective Teaching Techniques
Surgical trainers employed several specific techniques to enhance teaching effectiveness in robotic surgery, and this theme included sub-themes of clear verbal articulation with agreement, pre-performance face-to-face huddles, active feedback and explanation, and engaging questions.
Most prominent was the impact of clear verbal articulation with concise, simple, and mutually understood vocabulary and concepts, allowing the trainee to perform the action while communicating an important and timely principle. For example, during a low anterior resection (LAR) of the rectum (Case 4), effective communication from the attending surgeon both provides immediate direction and explained the rationale for specific camera horizon changes as the operative field moves from the left lower quadrant to the pelvis. In another LAR (Case 9), the trainer specifically asks their trainee to move, rotate and center the camera view relating to specific visualized structures and plane orientation as they are proceeding with medial to lateral dissection: “pull your camera a bit more…make this [plane] parallel…rotate the other way.” In several other instances the attending instructs their trainee, “push towards the sacrum” or “tip towards the head” communicating with their trainee clear and concise instruction about intended directionality. During a robotic lung wedge resection (Case 6), the attending surgeon directly instructs the trainee on how to proceed with stapling the lung parenchyma, utilizing concise language (e.g. “drop the elbow,” “rotate the stapler counterclockwise,” “advance/retract the stapler”) followed by affirmation when done correctly.
Another effective teaching technique observed in our data was a pre-performance face-to-face huddle. In this behavior, trainer and trainee raise their heads out of their respective consoles for a face-to-face exchange. (Figure 4) The exchange was typically verbal but at times involved demonstrative hand gestures, e.g. physically demonstrating how to align the stapler properly with respect to the colon and mesentery just before resection during an LAR:
Attending: Like this…Colon, [with the] mesentery down…[go] straight across…normally we go anti-mesenteric, but now go straight across. [tapping resident on shoulder to initiate “head out” interaction; gesturing with hands to demonstrate colon and mesentery, holding out two fingers to represent stapler coming straight across vs. “antimesenteric”] (Case 4, Figure 5)
In another example demonstrating how to orient the mesh in an inguinal hernia repair, the attending surgeon similarly initiates a face-to-face interaction and then gestures to demonstrate a teaching point:
Attending: The mesh is laying like this…here is the ML…it needs to [orient] like that… what I want you to do is grab the top and swing it like this. (Case 7, Figure 6)
Pre-performance huddles usually took place just before the start of a case for a preoperative debrief, but might also occur during the procedure, just before a critical step or when a concept is particularly challenging to explain verbally. They were notable in our observations as an important moment for teaching, communication, and reinforcing dyadic trust.
Active continuous feedback and explanation were also observed to be an effective teaching technique. Trainers provided ongoing commentary either verbally or through telestration as the trainee operated, rationalizing a certain technique, emphasizing the importance of a certain structure, or giving recurrent affirmations. One trainer’s utterances during a robotic inguinal hernia repair illustrate this sub-theme:
Attending: Yep. Big spreads. One deeper. Yep. Nice. Yes. Good. And so here you're not going to be able to get all the way to Cooper's because it's a direct, right?
Resident: Right.
Attending: But you can do some more. It's coming. Do what's easy.
Resident: It's so thin here. I'm trying to get a little more tissue.
Attending: You can pop pre-transversalis whenever you feel like you need to, because it doesn't really matter. Because when you get down here, they will become the same plane, right?
Resident: That's true. (Case 3)
In this instance, the attending surgeon provides multiple affirmations and explains why a particular dissection is not suitable, allowing the trainee to adjust their technique in real-time. This strategy maintains engagement for both trainer and trainee, facilitates the progress of the procedure, organically reveals the parameters of the dissection, and reduces the likelihood of the trainer taking control due to ongoing guidance.
The final sub-theme in effective teaching techniques involved utilization of open-ended questions to explore the trainee’s thought process and decision-making. This was frequently utilized when the trainee had control, but next steps were unclear, or the procedure was stalling:
Attending: What do you think?
Trainee: Sure.
Attending: Love your certainty. Are you SURE-sure?
Trainee: I was trying to get a little bit more posterior because I thought there was some more but ...
Attending: Some more what? Mesentery?
Trainee: Yeah. I think this side's fine. The right side I think is okay because I could see it decently well. It's the other side that I was struggling with.
Attending: Left posterior, okay.
Trainee: Yeah, like that fat at the tip, I was struggling to get the tension and stuff. Because I feel like that's lower than where we're going to staple across.
Attending: Could be. [Trainee continues dissecting] Okay, good. (Case 8)
This approach allowed the trainer to understand the trainee's rationale and offer guidance or corrections without taking over the operation.
Feedback Escalation
The second theme noted in our thematic analysis was Feedback Escalation, with stages specific to robotic surgery. (Figure 7) “Escalation” of feedback typically occurred when a trainee was unable to carry out a certain task, and was noted to be correlated with decreased trust, increased urgency, or situations in which a trainer was unable to adequately convey instruction verbally.
Feedback Escalation progressed through stages of 1) verbal feedback, 2) use of surgical telestration and on-screen guidance markers, 3) intraoperative "head-out" huddles, and 4) complete takeover of the console by the trainer, which might be either to demonstrate a specific technique, before returning control, or to complete the surgical task themselves. Generally, feedback escalation followed this stepwise progression. However, during particularly challenging tasks or when the trainer could not effectively explain a concept, it was common to skip steps. Accelerated escalation and skipping steps were observed with low trainer mLMX trust scores, while slower escalation was observed with high trainer mLMX trust scores.
The following examples illustrate Feedback Escalation during a robotic lung wedge resection, in two different contexts (Case 6). In the first context, the attending surgeon asked the trainee to control staple line bleeding. After verbal feedback and instruction, the trainee was unable to control bleeding because of mobile lung parenchyma. The attending took control of the console, demonstrated how to stabilize the lung parenchyma, and partially cauterized the staple line. They then gave control back to their trainee and the trainee was able to complete the task. This example showed accelerated escalation and skipping steps given the situation, demonstrative behavior on the trainer’s part, and then exhibition of “feedback de-escalation” by handing back control. In another context, the attending verbally instructed their trainee to use gauze to retract the lung. When the trainee was unable to retract appropriately, the attending then escalated to using on-screen markers to demonstrate where to apply the gauze and how to position the graspers. After multiple attempts, the attending took control and demonstrated the appropriate technique. The trainer then “de-escalated feedback,” handed control back to their trainee, and used on-screen markers until the trainee was able to emulate their technique.
Trust Fostering Behavior
A third major theme arising in our data described behaviors exhibited by trainees that promote trainer trust. Sub-themes included clarification of intent (verbally or physically) and closed-loop communication. Trust-fostering behaviors were notable in interacting with Feedback Escalation, to de-escalate from console takeover and regain trainee autonomy.
Intent could be verbalized along with physical pointing. For example, in an inguinal hernia repair, the trainee stated to the attending surgeon, “I am going to go here,” as they were fixing the mesh onto Cooper’s ligament during a robotic inguinal repair (Case 7), or “you probably want me to start in here?” while indicating with an instrument where the flap closure suture line might begin (Case 1). Physical gestures to indicate maneuvers before execution were also a common example of trust fostering behaviors that clarify trainee intent. Later in the same procedure, the trainee states, “I see this… and then I am going to do one here…and then I am going to pulley it up” pointing to the proximal edge of the flap and gesturing in a pulley motion before they close it. These statements allow for trainer affirmation and course correction, especially if a trainee is unsure of the appropriate steps.
In the sub-theme of closed loop communication, the trainee signals that they understood the trainer’s instruction by repeating it, sometimes with physical pointing. This method partially compensates for the lack for non-verbal cues typically present in laparoscopic and open surgeries. For instance, during another robotic inguinal hernia repair, the attending and trainee confirm mutual understanding of an anatomical structure:
Attending: See that? [utilizing on-screen pointers to indicate a structure] That’s the pseudosac, right there.
Resident: This edge, right here; I see it. [utilizing tip of instrument to outline the same structure on screen]
Attending: Yep. It's attenuated transversus… So that needs to go up, which is exactly what you're doing. Some people see that and think it's hernia sac and follow it. (Case 3)
This closed-loop communication confirms the trainee's understanding of the trainer’s reference. All the aforementioned actions were generally observed to preempt console takeovers and “de-escalate feedback.” In some instances, closed-loop communication takes place over an extended interaction, integrated with clarification of intent:
Attending: You see that? See your spot in the back where it connects?
Trainee: Yeah.
Attending: Yeah. So, get one jaw back there.
Trainee: Okay. [positions vessel sealer instrument]
Attending: There you go. That's right. Yeah.
Trainee: Ooh… That's firm though. [closing instrument without firing]
Attending: Is it?
Trainee: Yeah. It seems like it is. [continues to open and close instrument to indicate visual cues of tissue firmness]
Attending: I agree with that. So, let's see… So, what else?
Trainee: Either above, I can try taking it higher or ...
Attending: I don't think so. So, try taking… Is that tumor?
Trainee: I'm not sure. I mean… [tapping area of interest with instrument]
Attending: It might be. So cut just the peritoneum. [utilizing on-screen pointers to indicate area to cut]
Trainee: Like this right here? [pointing with instrument]
Attending: Yeah. Try that. (Case 8)
As a result of these trust fostering behaviors, the trainee maintains autonomy as the primary operating surgeon, even in situations of uncertainty.
{kind=link}
{kind=link}