Numerical results and analysis
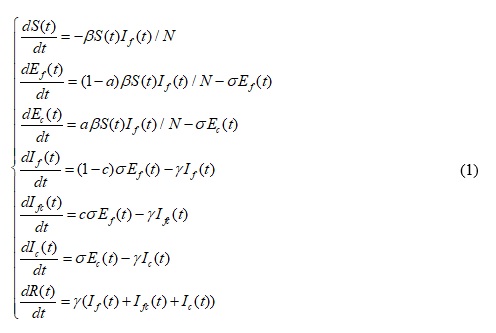
Using the SEfEcIfIcIfcR model with parameters in Table 1 and the data from the WHO, we show the numerical results of predicted confirmed cases number in the three countries, include the result under control-free and under practical control (Fig.2). The blue curve is the predicted confirmed cases number by fitting the early phase weekly data to an SEIR model. The black curve is the result by fitting the data to our SEfEcIfIcIfcR model. It is clear that the three maximum values of new weekly infected cases are up to about 290, 1,100, and 1,300 in Guinea, Liberia, and Sierra Leone, respectively, which are far more than the confirmed cases from the WHO (171, 364 and 565, in the same order). This result implies that the Ebola prevention and control measures are urgent and important. Evidently, the practical control measures in the three countries are effective.
Fig.2. Comparative between the fitting results of two models and the data from the WHO.
We also obtain the basic reproduction number of the system (1). The basic reproduction number under control Rc = (1 − a)(1 − c)β/γ by using method in [16]. The estimated parameters in the model are shown in Table 2. A larger value of a means that more efforts toward high-risk individuals in the country were made thanks to the pre-infected measures, such as common knowledge of Ebola, laboratory capacity, effective quarantine aimed to probable and suspected patients, contact tracing and Community Care Centre (CCC). The results show that Liberia’s pre-infected measure is the most efficient (a = 0.5832), follows by Sierra Leone (a = 0.3696), and then Guinea (a = 0.1827). Meanwhile, a larger value of c means that more efforts toward infectious individuals were made thanks to the post-infected measures, such as laboratory capacity, effective quarantine aimed at patients with a definite diagnosis, and the number of safe burial teams for dead patients, contact tracing team number, and ETU beds number. It is clear that the post-infected measures in Liberia (c = 0.3278) worked better than those Sierra Leone (c = 0.1281) and in Guinea (c = 0.1091), and Guinea achieved the worst outcome in terms of pre-infected and post-infected control measures.
Table 2. The results of key parameters in the model.
To show the impact of the two control parameters, we determine the numerical results of the relation between the predicted accumulated numbers in the model and the two control parameters. In Fig.3, the predicted value is a decreasing function of the two parameters. For the three countries, the predicted values of the accumulated infected number will sharply decrease when the two parameters decrease in the field with small a and c. It is shown that the estimated values of Guinea lie in the sharply decreasing field while those of Liberia lie in the gently decreasing field. This means that Liberia conducted a more efficient control strategy and Guinea’s control strategy needed improvement.
Fig.3. The predicted accumulated confirmed cases in the model vs. a and c is the control parameters (“*” in the figure is the fitting value in Table 2).
We further studied the sensitivity of parameters a and c. We fixed one parameter at the values shown in Table 2 and varied the other parameter. As shown in Fig.4 and in Table 3, we can find that Guinea had the largest relative rates of change with respect to a and c, which means that small improvement in the control strategy will sharply decrease the accumulated infected number.
Table 3. The relative rate of change in the three countries.
Fig.4. The sensitivity of parameters a and c in the three countries.
Based on the information on EVD spread control measures in the situation reports provided by the WHO, we obtain the following data: the number of Ebola treatment units (ETU) beds, the number of suspected cases and probable cases, which we defined as the quarantine number before infection, and the number of safe burial teams. First, we conduct a correlation analysis among the three measures above and the weekly EVD increase rates in Guinea, Liberia and Sierra Leone, respectively (Fig.5, Fig.6 and Fig.7). The new confirmed case increase rates are all negatively correlated with the three measures, with a statistically significant difference. The number of weekly ETU beds, the quarantine number before infection, and the number of safe burial teams are modeled separately with the increase rates of new confirmed cases, and the results of which achieve a goodness of fit. R2 are 0.690 (P < 0.001), 0.848 (P < 0.001), and 0.772 (P < 0.001), respectively. Moreover, to know which of the three measures has the greatest impact on the increase rates of new confirmed cases, we conduct a multivariate linear regression analysis to identify the most relevant factors against the overall backdrop. The results are shown in Table 4. The absolute values of the standardized coefficients of quarantine measures before infection is the largest (ε = 1.012, P < 0.01), that of increasing the ETU beds number follows (ε = 0.432, P < 0.05), and that of increasing the safe burial teams is the smallest (ε = 0.385, P < 0.05).
Fig.5. The correlation analysis between established ETU beds and the weekly EVD increase rates in Guinea.
Fig.6. The correlation analysis between quarantine before infection and the weekly EVD increase rates in Liberia.
Fig.7. The correlation analysis between safe burial teams and the weekly EVD increase rates in Sierra Leone.
Table 4. Standardized coefficients of the three measures.
All of the three measures have a favorable linear relationship with the increase rates of new cases. The results of multivariate linear regression analysis indicate that expanding the quarantine before infection is the most effective control measure. The following figures demonstrate the results above. Apparent differences are observed in the quarantine number before disease among the three countries (Fig.8, Fig.9 and Fig.10). Within the statistical data we obtained, the ranking of the maximum proportion of the quarantine number before infection of the total quarantine number is as follows: Liberia (79.31%) > Sierra Leone (31.35%) > Guinea (25.62%), and the differences among the three countries are all statistically significant (P < 0.05).
Fig.8. The quarantine number before EVD outbreak in Guinea.
Fig.9. The quarantine number before EVD outbreak in Liberia.
Fig.10. The quarantine number before EVD outbreak in Sierra Leone.
{kind=link}
{kind=link}