Prednisone and dexamethasone are both oral CS therapies recommended for treating patients with moderate to severe asthma exacerbations. While prednisone is more commonly used [27], studies in children and adults have shown that dexamethasone has a similar safety profile and efficacy in terms of reducing relapse rates, hospitalizations, symptoms and time to return to normal activity [29, 30, 33-35]. Moreover, its long half-life and shorter treatment duration have proven popular among patients, caregivers and clinicians, especially in children with acute asthma. Dexamethasone is a more potent GR agonist than prednisone [28]; however, whether it is more effective in reducing inflammation is less well understood. Here, we examined the anti-inflammatory effects of these two CS agents in vitro and found that dexamethasone was both more potent and more effective than prednisolone. As such, our data suggest that treating exacerbating asthmatics with dexamethasone may result in better control of symptoms and/or severity of disease, aspects of asthma mediated by persistent inflammation.
Studies comparing the effectiveness of standard dose regimes of dexamethasone (12 -16 mg/day, 1-2 days) to prednisone (60 mg/day, 5 days) found no difference in asthma relapse rates within two weeks [33-35]. These studies, however, failed to examine longer time points or differential CS effects on cellular or cytokine responses. Our study shows that dexamethasone significantly decreased IL-13 mRNA at a 10-fold lower concentration (10-9 mM) than prednisolone. IL-5 appeared to be generally less CS sensitive, with significant suppression observed only at 10-8 mM dexamethasone. However, at the highest concentration examined (10-7 µM), still physiologically relevant [44], both CS agents almost completely suppressed IL-13 and IL-5 mRNA levels. This result indicates that in vivo type 2 cytokines are likely sufficiently controlled with an optimal dose of either prednisolone or dexamethasone and, in line with other reports, are anticipated to reduce the proportion of CD4+ T cells expressing IL-4 and IL-5 [50]. However, we recently showed that the suppressive effect of dexamethasone on IL-13 was reversed after activation unless cells were continuously exposed to dexamethasone [45], suggesting the effect could be temporary. The lack of increase in IL-10 or IL-17 following dexamethasone treatment [45], coupled with our new data showing that dexamethasone reduced IFNg mRNA levels (Table 1), indicates active suppression of type 2 cytokine transcription, rather than shifting Th2 cells toward a Th1, Th17 or T regulatory cell phenotype.
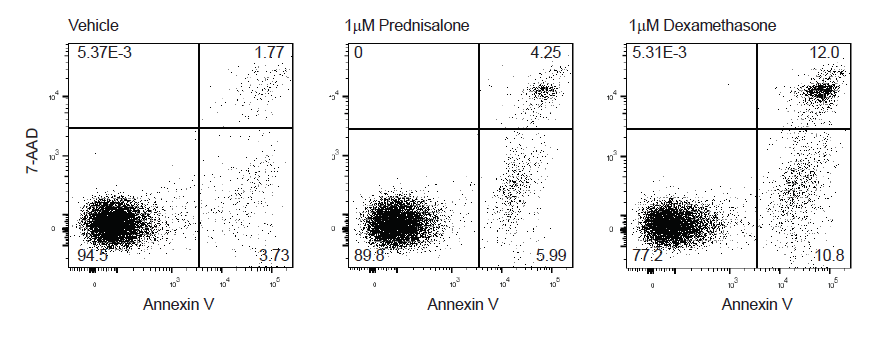
Type 2 cytokines mediate many features of asthma and therapies blocking their action are effective and are now recommended as frontline controllers in severe asthma [24]. Attention, however, is now turning toward therapies that reduce the proportion and/or development of type 2 cytokine-producing cells with the long term hope of actually modifying or curing asthma [51]. Circulating Th2 cells are an important aspect of immune memory and their level controls a patient’s susceptibility to respond to allergens and the development of persistent symptoms. For this reason, we examined differences in the ability of these two CS agents to induce Th2 cell apoptosis. We found that dexamethasone was superior to prednisolone in driving apoptosis (~10-fold more effective) - no matter the concentration added, prednisolone was never able to induce apoptosis to a similar degree as dexamethasone. These results suggest prednisolone is a partial agonist, relative to dexamethasone, similar to previous studies showing this in terms of gene expression [52] and the ability of dexamethasone to enhance prednisolone-induced cytotoxicity [53].
Prednisolone failed to match the degree of dexamethasone-induced apoptosis, but was equi-effective in cytokine suppression. This difference may be due to mechanism(s) of action. Corticosteroid suppression of IL-5 and IL-13 has been shown to be due to GR interfering with transcription factors binding to the promoter of these type 2 cytokine genes [14], while GC-induced apoptosis has been associated with induction of pro-apoptotic genes such as BIM (BCL-2-interacting mediator of cell death) [54]. Our results suggest that dexamethasone more effectively induces pro-apoptosis genes than prednisolone. Indeed, others have shown differential effects of various steroids on gene expression; in airway cells dexamethasone, fluticasone, ciclesonide (and others) were equally effective in driving the expression of some genes (GILZ, p57kip2), but not others (PDK4) [55].
Clearly, studies are needed to examine the effect of dexamethasone compared to prednisone in patients experiencing asthma exacerbation, but this is challenging since dexamethasone is more often prescribed to children and prednisolone is the oral CS of choice in adults. A few studies have compared these two CSs and found they were associated with similar rates of relapse and hospitalization within 10-14 days [34, 35], providing little rationale to recommend a change in prescribing habits. Those studies, however, did not assess whether dexamethasone had a stronger suppressive effect on immune cell responses such as the degree of Th2 cell apoptosis. There is evidence to suggest that stronger GR agonists provide better outcomes; Demirca et. al. showed type 2 cytokine expression at day 7 following ex vivo activation of peripheral blood mononuclear cells was higher in patients who received oral methylprednisolone post-exacerbation compared to those who received the more potent fluticasone propionate [56]. Our mechanistic data suggest that the higher potency dexamethasone induced more Th2 cell apoptosis than the weaker agonist prednisone. In vivo, dexamethasone may be better able to eliminate Th2 cells thereby reducing persistent symptoms driven by type 2 inflammation and could result in fewer sub-acute relapses and/or repeat exacerbations. As such, our in vitro data beseech clinical centers to perform head-to-head comparisons of these two CS agents to determine their relative in vivo effect on type 2 inflammation and persistence of symptoms.
Since corticosteroid withdrawal studies have shown that suppression of type 2 inflammation requires continuous exposure to steroid [45, 57, 58], therapeutic approaches aimed at eliminating Th2 cells may provide more sustained repression of allergic responses. Th2 cells are highly differentiated with a strong ability to survive, mediated through expression of the anti-apoptotic factor BCL-2 [59, 60]. The BCL-2 inhibitor ABT-199, in clinical trials for leukemia [61], was also shown to reduce the level of airway eosinophils and Th2 cells in a mouse model of asthma [62]. Huang et. al. showed that elimination of Th2 cells (using an antibody against CRTh2) resulted in significantly fewer eosinophils and lower levels of type 2 cytokines and chemokines in the blood, lymph nodes and lung in a mouse model of asthma [63]. Ultimately, therapies targeting development of Th2 cells, such as those blocking the IL-4Ra or the cytokine TSLP [64, 65], may prove the most effective in reducing persistence of asthma symptoms.
Women and men respond differently to acute asthma. For example, women are more likely to relapse following an asthma exacerbation than men [37]. Furthermore, the female sex hormone progesterone has affinity for the GR [41]. As such, we examined whether progesterone could dampen the ability of CS to induce Th2 cell apoptosis and its mechanism of action. We found that progesterone (1mM, considered to be a physiologic level during pregnancy [41]), interfered with both prednisolone and dexamethasone and that the effect was identical if hormone was added in combination or as a pre-treatment. The Th2 cell line (CCRF-CEM) and primary Th2 cells had no PGR mRNA and no production of PIBF1 mRNA in response to progesterone, indicating that the effect was not due to activation of nuclear progesterone receptors [46]. We did, however, find that progesterone reduced the level of FKBP5 mRNA, a gene known to be induced by GC exposure and GR binding to its promoter [48, 49]. As such, our data suggest that progesterone antagonizes GC:GR signaling, rather than acting through its own receptor. This finding is in line with Guo et. al., who showed that treating murine NK cells with the progesterone analog P4, in the presence of PGR blockade, antagonized GR signaling and reduced IFNγ and CD69 expression following CpG/IL-12 stimulation [66]. Progesterone was also shown to antagonize dexamethasone-induced apoptosis of murine thymocytes [67]. Collectively these studies support our hypothesis that circulating progesterone levels may influence the efficacy of CS action in vivo, which could explain why some women experience worse symptoms at times when progesterone levels are elevated [38, 39] and are more likely to be diagnosed with severe asthma [36].
Dexamethasone is a long-acting CS (36-72 hour half-life) with 30 times more GR activity than hydrocortisone. Due to these factors, long term dexamethasone treatment is associated with serious side effects, such as suppression of the hypothalamic-pituitary-adrenal (HPA) axis, so is generally reserved for treating acute symptoms like exacerbations of asthma [27]. Prednisolone is less potent (4 times the activity of hydrocortisone) and is shorter acting (12-36 hour half-life) [27], so historically it has been used as a controller medication. In 2012, due to the known side effects of long term oral steroid use, the GINA guidelines downgraded the use of oral CS in chronic asthma and recommend them only if other controllers, such as anti-IgE and anti-IL-5, were not available or did not work [68]. Nevertheless, a recent study of severe asthmatics reported a third of their study population was using oral prednisone, with an average duration of 4 years and mean dose 17.5 mg/day [69]. The ranges of oral prednisone prescribed vary greatly from very low (1 - 7.5 mg/day) to higher doses (10 - 40 mg/day) [68]. Though less than recommended for exacerbation (60 mg/day) [34, 35], these doses equate to in vitro concentrations of ~ 0.3 - 0.8 mM (7.5 - 17.5 mg/day). In light of our data, the dose range of prednisolone for chronic use may be sufficient to suppress type 2 cytokine levels, but relatively inefficient as an inducer of apoptosis, particularly in women. These data indicate that inhaled CS formulations of higher affinity GR agonists, such as fluticasone furoate [70], may also be effective in eliminating Th2 cells and suggest this should be examined in future studies.
{kind=link}
{kind=link}
{kind=link}