This study provides evidence supporting the association between IR and sleep apnea severity. Our results highlight the potential for pulmonary IR to play a important role in the development and progression of sleep apnea. The pulmonary IR has garnered significant attention in respiratory research due to its impact on lung function. The presence of insulin receptors in the lungs highlights the direct influence of insulin, but IR hampers this response, leading to compromised pulmonary performance. This study establishes a link between IR and the severity of sleep apnea, especially in cases of moderate and severe AHI. Thus, these results emphasize the importance of recognizing IR as a potential contributing factor to sleep apnea risk and suggest the plausibility of localized pulmonary IR.
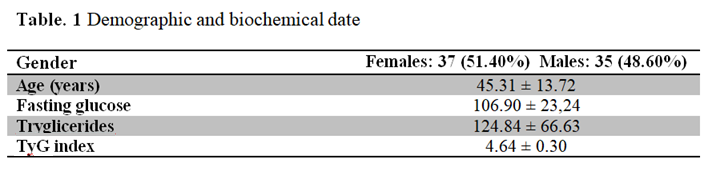
TyG index can serve as a practical alternative of IR measurement, and previous studies showed that a higher TyG index showed a higher risk of obstructive sleep apnea.8 Chronic intermittent hypoxia, a hallmark pathophysiological consequence of sleep apnea, is a primary mechanism underlying the development of IR.9 Additionally, sleep fragmentation and deprivation may also contribute to the pathogenesis of IR in this context.10 Moreover, genetic and epigenetic factors play a significant role in modulating the relationship between the TyG index and sleep apnea.11 Our study evaluated the correlation between IR, using the TyG index, and sleep apnea. We employed logistic regression analysis to investigate whether IR was a risk factor for sleep apnea, adjusted for age and gender. Our findings revealed a significant association between the TyG index and sleep apnea.
The ESS, a self-reported questionnaire designed to gauge the propensity for napping during routine activities, has become the gold standard for quantifying daytime sleepiness in clinical and research settings.12 The ESS is a concise, self-administered questionnaire comprising eight items, designed to quantify daytime somnolence across various levels of arousal. With a total score ranging from 0 to 24, a score of 10 or greater is indicative of excessive daytime sleepiness, a clinical hallmark of numerous sleep disorders.13 Our study demonstrated a significant association between the ESS and IR, independent of gender and age. The ESS has been widely employed to assess subjective daytime sleepiness in other studies.14
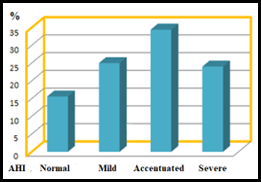
The AHI, calculated as the sum of hypopneas and apneas per hour of sleep, is the gold standard for quantifying the severity of sleep apnea. AHI values categorize sleep apnea into mild (5–14 events/h), moderate (15–29 events/h), and severe (> 30 events/h) categories.15 Hypertriglyceridemia is strongly linked to IR and can mask the underlying impact of AHI on insulin sensitivity. The lipolytic action of insulin, coupled with increased sympathetic tone induced by arousals and intermittent hypoxia associated with sleep apnea, contributes to the development of dyslipidemia and further exacerbates IR.16 Our findings align with a growing body of literature that underscores the strong association between sleep apnea, as quantified by the AHI and IR. Consistent with previous studies,17,18 we observed a correlation between increasing AHI severity and the frequency of IR. The significant positive association between moderate and severe AHI and IR, in particular, highlights the potential clinical implications of this relationship.
The ODI is calculated as the number of oxygen desaturations of ≥ 3% (over the last 120 seconds) that lasts for at least 10 seconds per hour of sleep, is a commonly used metric in sleep medicine. However, the ODI has several limitations, including its reliance on an arbitrary desaturation threshold and its inability to accurately reflect the severity or frequency of hypoxic events. Furthermore, the ODI may be influenced by factors such as arousal thresholds and the presence of underlying medical conditions.19 Our study demonstrated a clinically significant link between an ODI of 10 or more events per hour and IR.
Thus, our study underscore the relationship between IR and sleep apnea, reinforcing the notion that pulmonary IR may play a pivotal role in the development and progression of this disorder. The presence of insulin receptors within the lung tissue highlights the organ's direct susceptibility to insulin's influence. However, impaired insulin sensitivity within the lungs can lead to compromised pulmonary function, ultimately contributing to the severity of sleep apnea. The significant association observed between IR, as assessed by the TyG index, and sleep apnea severity, particularly in cases of moderate and severe AHI, further supports this hypothesis. These results emphasize the importance of considering IR as a potential risk factor for sleep apnea and suggest the need for a more comprehensive approach to managing this condition, encompassing both respiratory and metabolic aspects.
{kind=link}
{kind=link}
{kind=link}