Nuclear physics methods have been instrumental in improving cancer radiotherapy using accelerated charged particles (protons or heavier ions). Charged nuclei have indeed a favorable depth-dose distribution in the human body thanks to the Bragg peak1. Therapy with accelerated 12C-ions is currently ongoing in fourteen centers worldwide2 and, even if more expensive than proton therapy, adds biological advantages to the physical benefit of the Bragg peak3. Particle therapy is, however, much more sensitive to uncertainties in the beam range than conventional X-rays, exactly because of the high dose deposited in the Bragg peak4. Several techniques are available to monitor the beam range exploiting the nuclear interactions of the ions in the tissue5, including PET6. PET in carbon ion therapy exploits β+-emitting isotopes 11C and 10C produced by the nuclear fragmentation of the therapeutic stable 12C beam in the patient’s body. The method was extensively tested during the carbon ion therapy pilot trial at GSI in Darmstadt7, then at HIT in Heidelberg8 and more recently at CNAO in Pavia9. However, the counting rate from projectile fragments is low, the activity peak is largely shifted with respect to the Bragg peak because the particle range of the isotopic fragments of 12C depends on their mass, and the image analysis has been mainly performed off-line. Therefore, PET in 12C-ion therapy remains marginal and is not really able to reduce the range uncertainty as desired.
Most of these problems can be overcome using RIB rather than stable beams for therapy. RIB are generally acknowledged as the main tool to address the most important modern questions in nuclear physics, as they allow the study of nuclei at extreme conditions10–12. In cancer radiotherapy, RIB have the same biological effectiveness of the corresponding stable ions beams13,14 but can increase the PET signal/noise ratio by approximately an order of magnitude, reduce the shift between the activity and dose peaks, and mitigate the washout image blur with short-lived isotopes (e.g.10C) and in-beam acquisition15,16. The reduced uncertainty in range allows a shrinkage of the tumor margins around the clinical target volume (CTV), and this can lower toxicity for both serial or parallel organs-at-risk (OAR)17. Attempts to use RIB in cancer therapy started already in the 80s during the heavy ion therapy pilot project at the Lawrence Berkeley Laboratory (CA, USA)18, but they were always hampered by the low intensities of the secondary beams produced by fragmentation of the primary ions used for therapy (for an historical review see ref.19). Research at modern high-intensity accelerators that can produce RIB with intensity sufficient for therapeutic treatments20 would pave the way to PET-guided heavy ion treatments. One of these facilities is GSI/FAIR in Darmstadt (Germany)21, where we started the BARB (Biomedical Applications of Radioactive Ion Beams) project whose goal was to perform the first in vivo tumor treatment with RIB15.
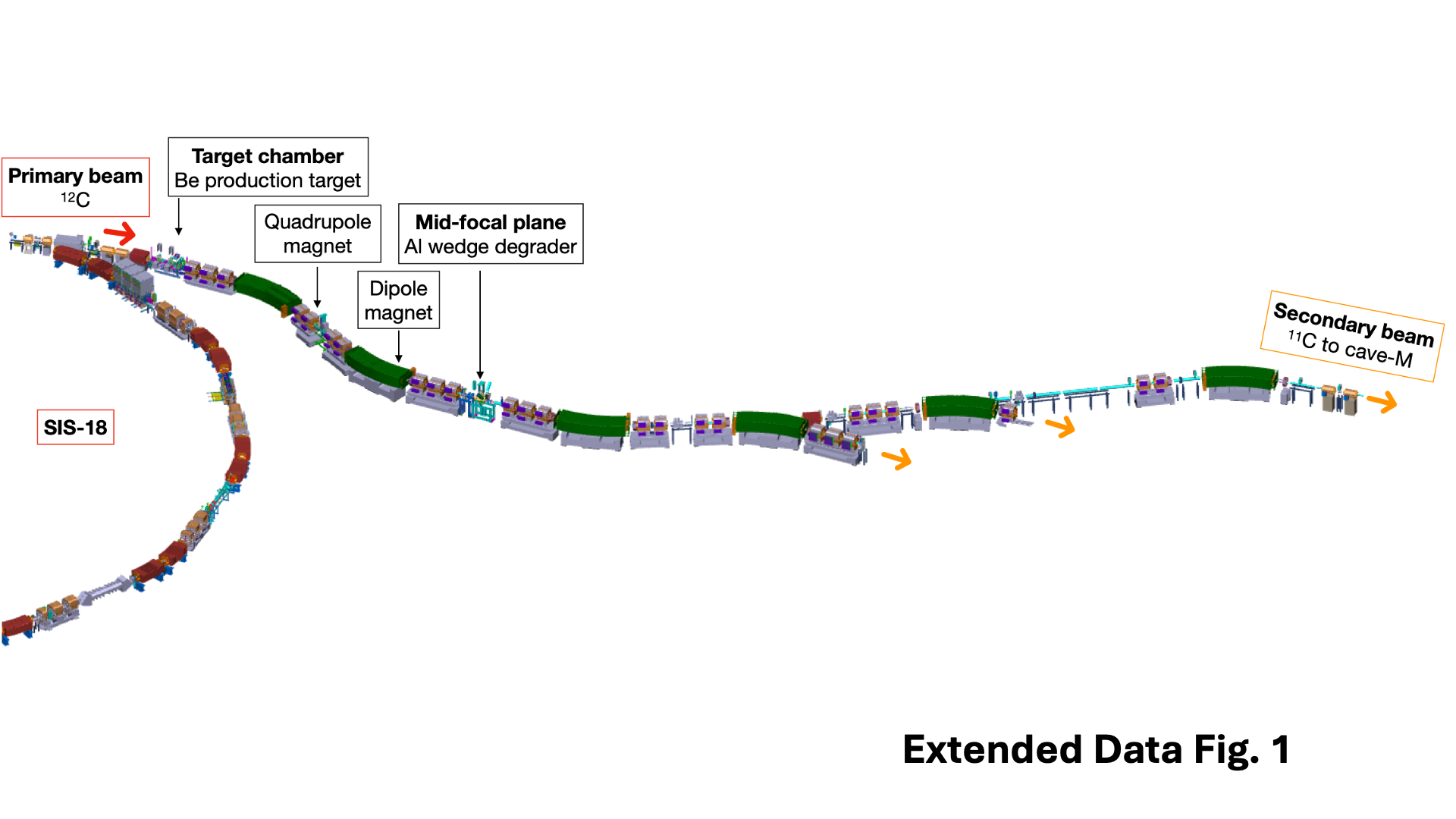
Within BARB, we have already reported the RIB imaging resolution in phantoms22,23 and transported the beam from the fragment separator (FRS) to the medical vault (Cave M, where animal experiments are possible) at the GSI accelerator facility24 (Extended Data Fig. 1). In Cave M we have then enabled the reproducible installation of the portable small-animal SIRMIO in-beam PET scanner25, built by the Ludwig-Maximillian-University (LMU) group in Munich for in vivo range verification in pre-clinical particle therapy experiments. The SIRMIO PET scanner is based on 56 scintillator blocks of pixelated LYSO crystals. The crystals are arranged providing a pyramidal-step shape to optimize the geometrical coverage in a spherical configuration26. Inside the detector it is possible to accommodate an anesthetized mouse in vertical position using a custom 3D-printed holder for simultaneous irradiation and real-time PET imaging, also developed at LMU. The mouse model used in this study is a syngeneic LM8 osteosarcoma implanted in the C3H mouse neck27. Osteosarcoma is a very radioresistant tumor28 and for this reason it is a typical candidate for treatment with accelerated 12C-ions29. Figure 1A shows µCT images of the tumor growth and the actual visible tumor in the neck. In Fig. 1B we show the contouring of the individual gross tumor volumes (GTV) of the different mice used in the experiments. By summing up all the tumor profiles and smoothing the resulting outline, we have contoured a universal CTV applied to all mice in this study. The proximity of the CTV to the spinal cord makes high precision and online guidance necessary to avoid radiation myelopathy30. Measured endpoints were tumor growth, spinal cord toxicity, and washout rate of the radioactive signal from the tumor. We elected to use 11C projectile even if our previous experiments22,23 show that the highest range resolving power can be achieved with short-lived isotopes such as 10C or 15O. We preferred to use carbon, which is already used in many clinical facilities, rather than oxygen, and the intensity of N-2 isotopes such as 10C is too low for very high-dose single-fraction treatment. The goal of the experiment was to demonstrate for the first time the ability to use a 11C-ion radioactive beam to achieve full tumor control of a radioresistant tumor, such as osteosarcoma, proximal to an OAR, while maintaining low toxicity thanks to real-time PET image guidance.
The BARB beamline
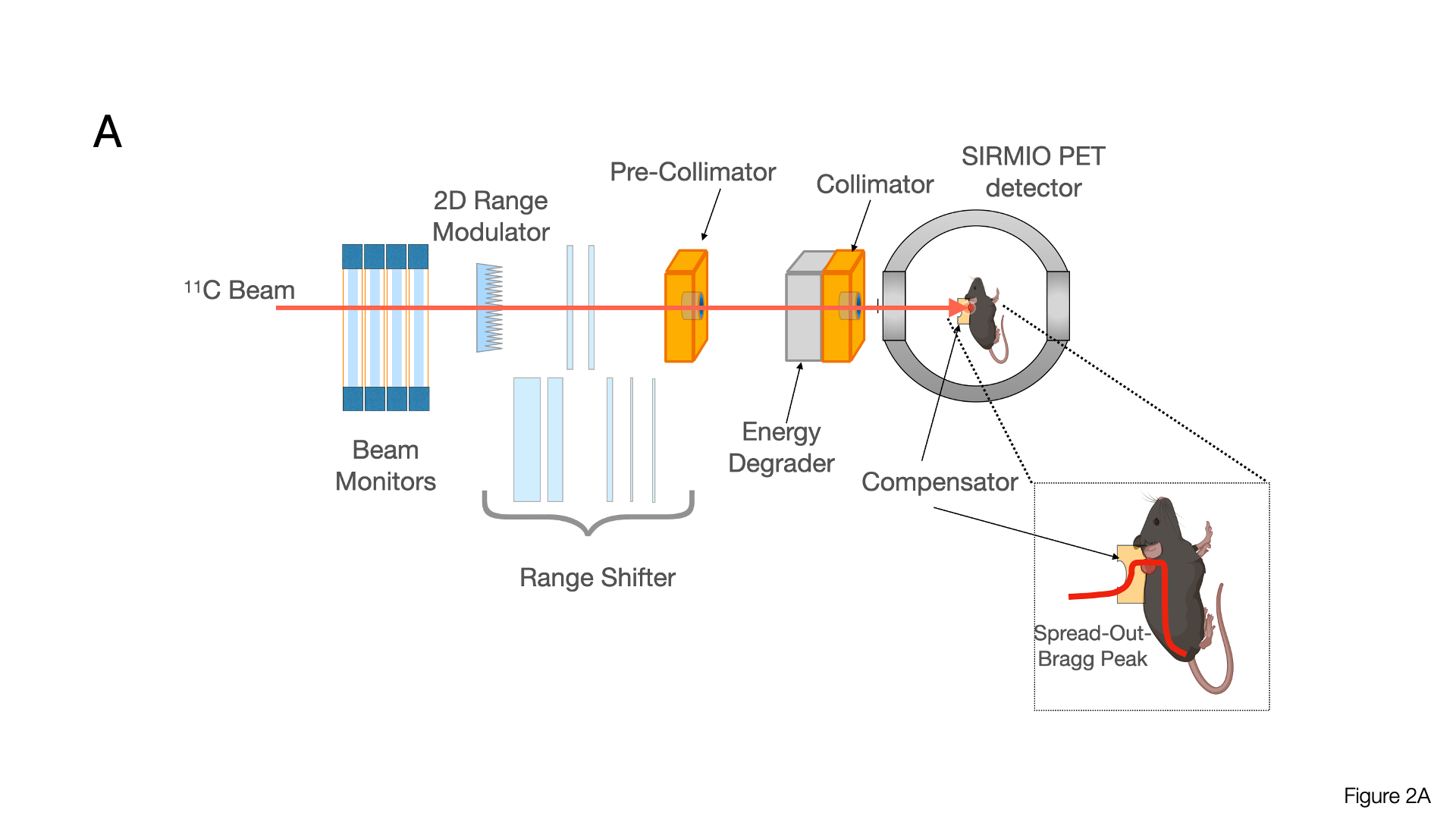
Figure 2 shows the full BARB beamline prepared in Cave M at GSI and photographs of different components. The secondary beam of 11C comes from the FRS31 (Extended Data Fig. 1). The primary intensity of the 12C-ion beam in the SIS18 at 300 MeV/u was 1.6⋅1010 particles/spill and the intensity of 11C-ions in Cave M entrance was 2.5⋅106 particles/spill. To allow a longer online PET acquisition time, we used a short spill duration of 200 ms and a relatively low duty cycle with a repetition rate of 3 s (see Extended Data Table 1 for a summary of all the parameters).
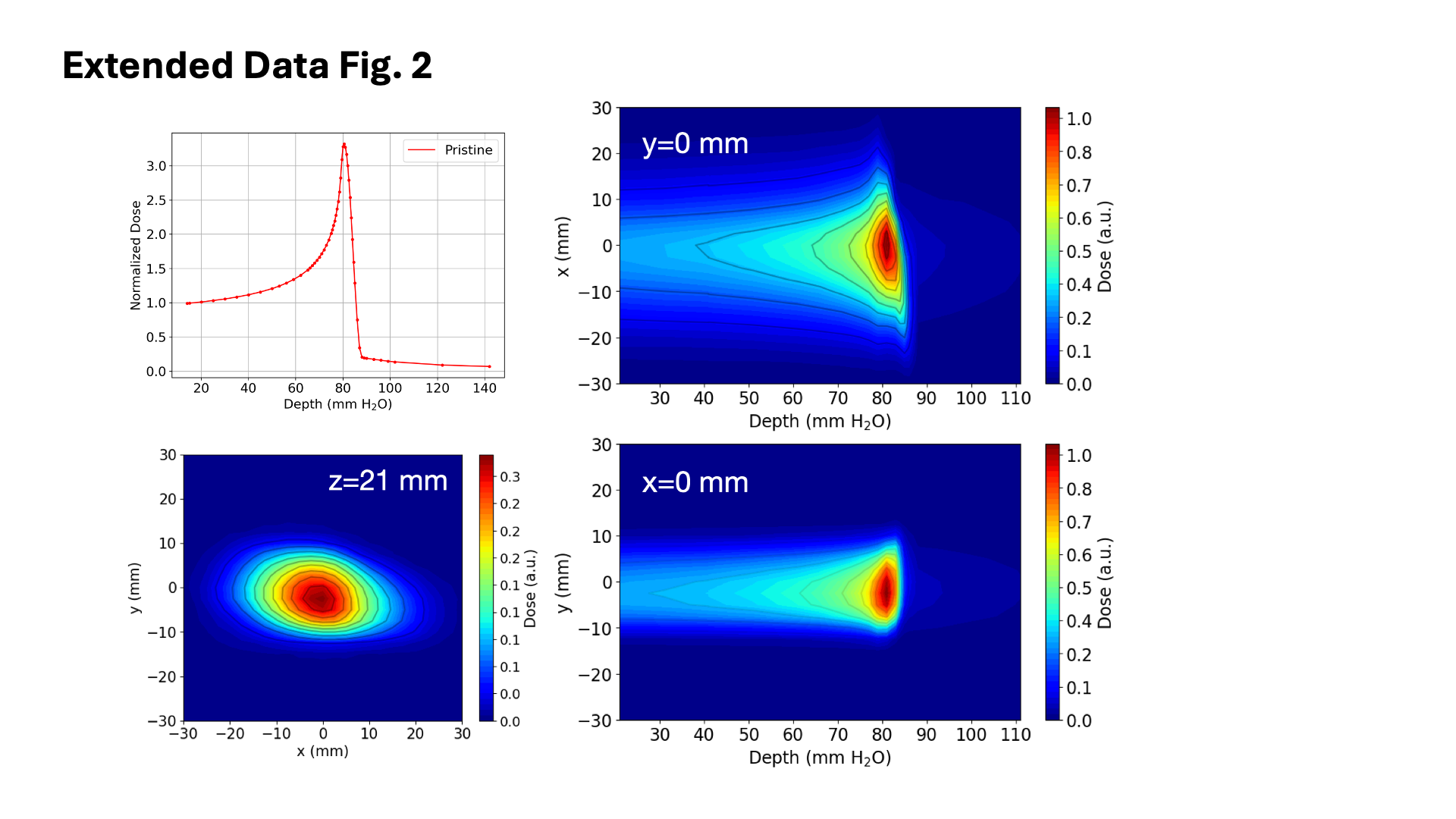
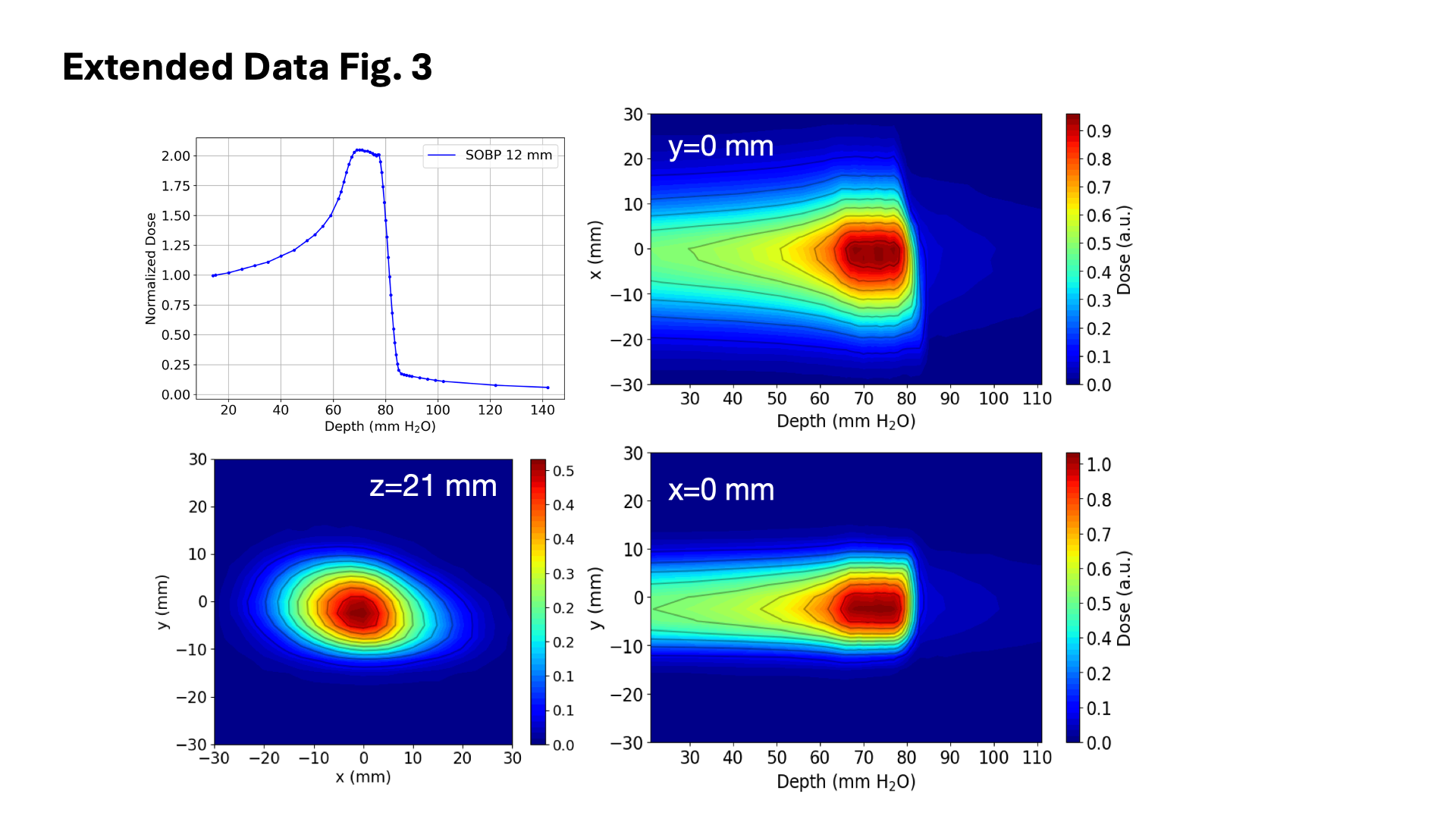
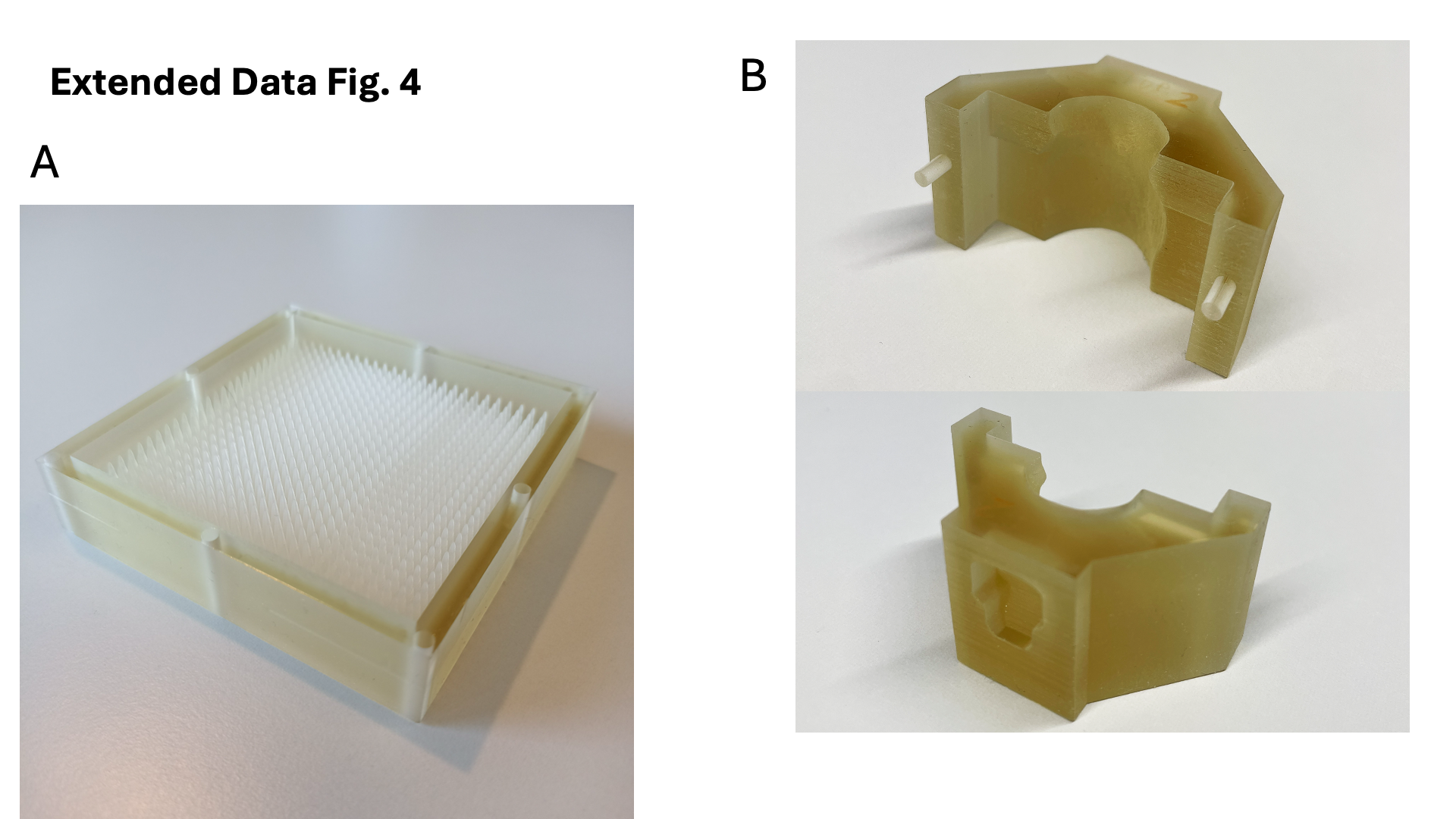
Measured pristine 11C-ion Bragg curve is shown in Extended Data Fig. 2. To cover the full CTV, the pristine Bragg peak has to be extended to produce a Spread-Out-Bragg-Peak (SOBP). The measured SOBP is shown in Extended Data Fig. 3. The SOBP was formed by a 3D-printed range modulator (Extended Data Fig. 4A) from a 2D scan of the monoenergetic pencil beam.
The distal field contour was modulated to the tumour CTV (Fig. 1B) by a 3D-printed plastic compensator collar (Extended Data Fig. 4B). We measured a dose-rate around 1 Gy/min in the tumor that was covered by the SOBP at the same dose. A total of 32 mice were irradiated with either 20 or 5 Gy.
Activity maps
In BARB we use real-time PET imaging to monitor the RIB dose delivery. A FLUKA32 Monte Carlo simulation of the beam reaching the tumor inside the SIRMIO PET scanner is shown in Fig. 3A-B along with the activity distribution image measured online (Fig. 3C) with 11C-ions by the PET scanner and overlayed on the µCT scan of the animal under irradiation. Measured activity and calculated positron annihilation profiles, integrated along the x-axis and displayed along the beam direction (z-axis), are shown in Fig. 3D along with the 1D dose profile in the z-direction. Even if the dose and the activity are deposited by the same ion in this experiment, the 11C beam momentum spread shifts the activity beyond the dose fall-off. A shift of approximately 2 mm is observed between the measured activity and simulated positron annihilation map peaks, with measured values closer to the actual dose fall-off. The depth at 80% dose fall-off matches the simulated activity peak. Supplementary video 1 shows the build-up of the measured PET signal vs. irradiation time in sagittal and transversal views. Individual images of all mice are shown in Supplementary Fig. 1. The tumour is very close to the spinal cord, and in-beam PET image was used to check that the SOPB was not covering the spine. For all animals (Supplementary Fig. 1) the peak activity was not inside or beyond the spinal cord, so no range correction by adjusting the degrader thickness (Fig. 2) had to be applied.
Tumor control
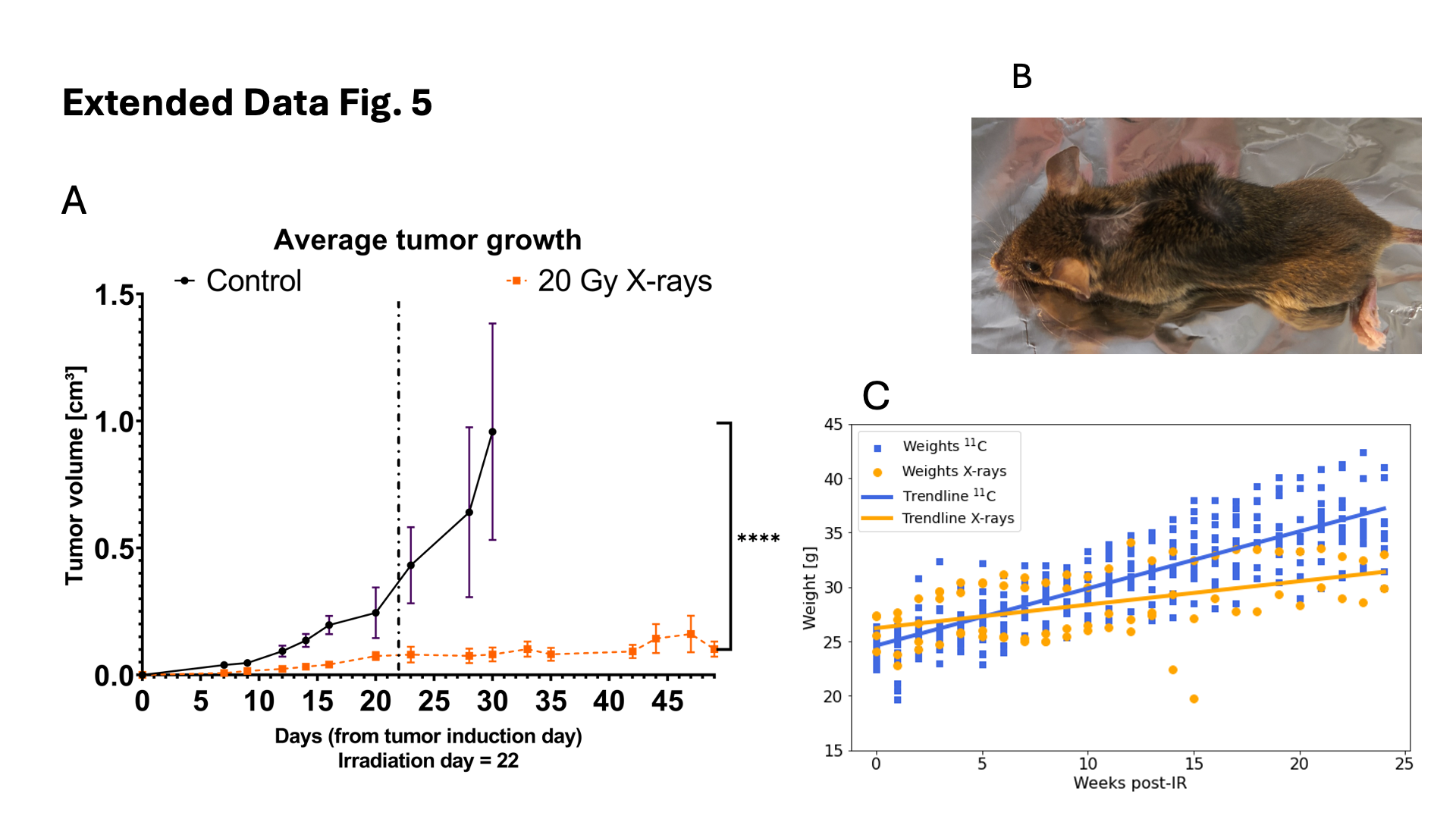
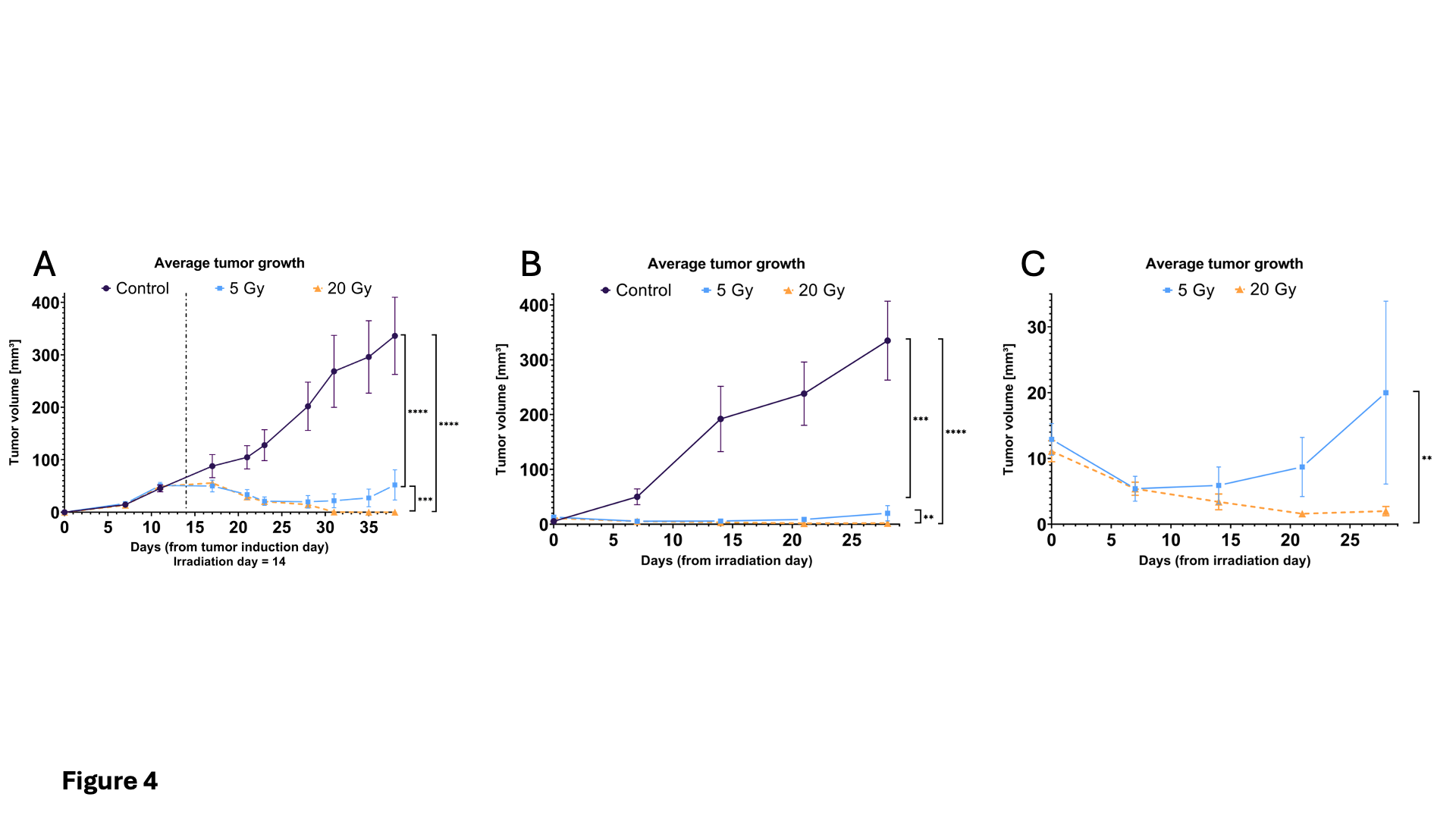
Tumor sizes of irradiated and control tumor-bearing animals were measured for four weeks after the day of irradiation using caliper or µCT. Results shown in Fig. 4 demonstrate complete tumor control after 20 Gy and prolonged tumor growth delay after 5 Gy, with evidence of recurrence after 2 weeks. Full tumor control was also achieved with 20 Gy X-rays (Extended Data Fig. 5). The data are compatible with a complete coverage of the tumor target for all animals. Recurrence at the lower dose is expected considering the high radioresistance of the osteosarcoma.
Toxicity
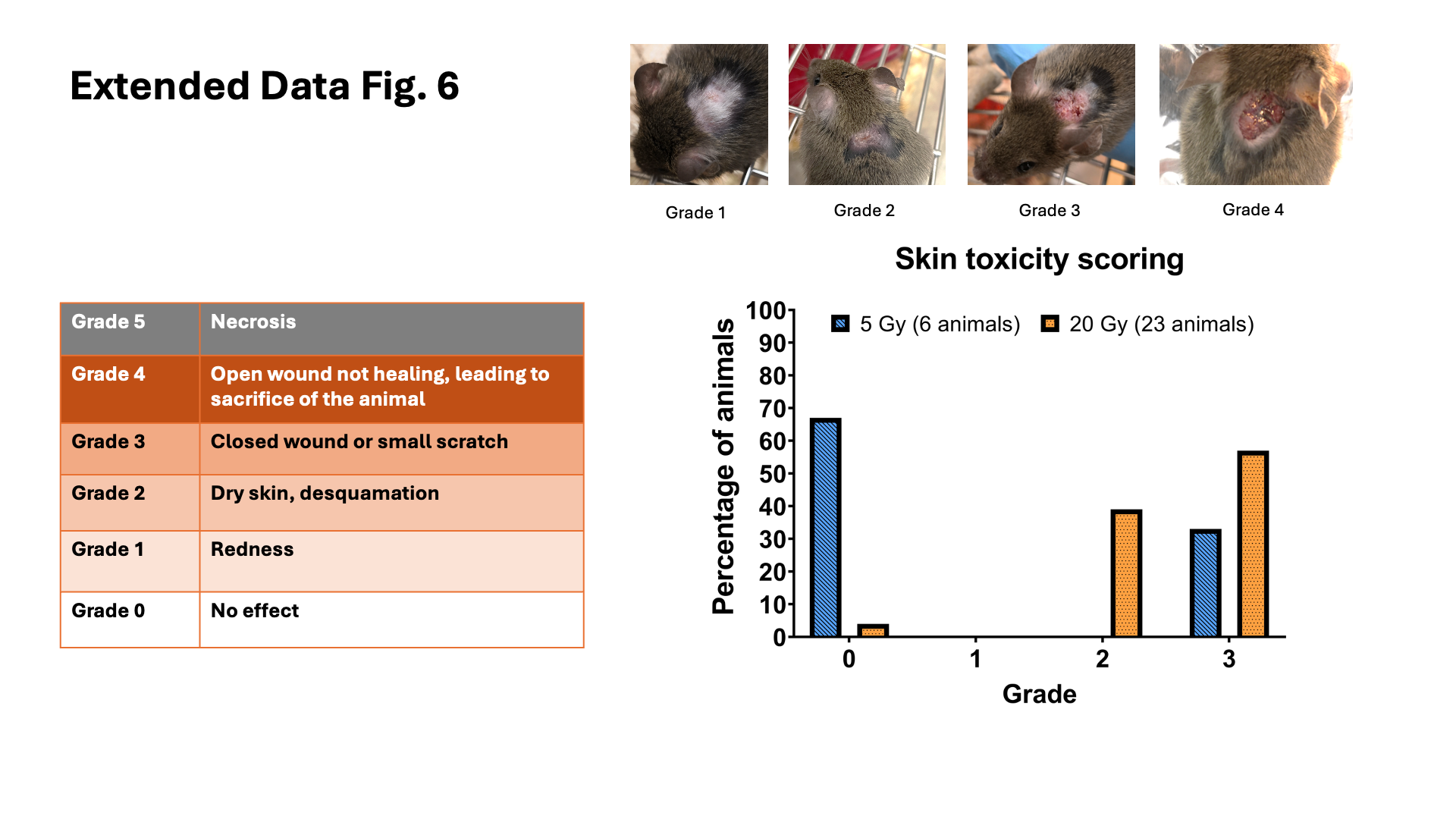
Skin toxicity scoring in the tumor-bearing controls was complicated by the growth of the tumor that caused superficial lesions. In irradiated animals, all of them bearing small tumors post-irradiation, skin toxicity was radiation-induced as shown in Extended Data Fig. 6. No animals showed skin toxicity grade > 3.
Being the tumor very close to the cervical area of the spinal cord, main expected toxicity was radiation-induced myelopathy. However, none of the animals exposed to 11C-ions presented severe morbidity such as forelimb paralysis or pronounced kyphosis. Extended Data Fig. 5 and Supplementary video 2 show the toxicity after X-rays, which is much more severe than for 11C-ions. Animals suffered severe weight loss due to impaired feeding, ostensibly caused by damage to the esophagus, and grade 3 kyphosis, caused by cervical myelopathy as expected from previous experiments30. This toxicity is related to the X-ray dose that, unavoidably, was received by the organs behind the tumor in the neck region.
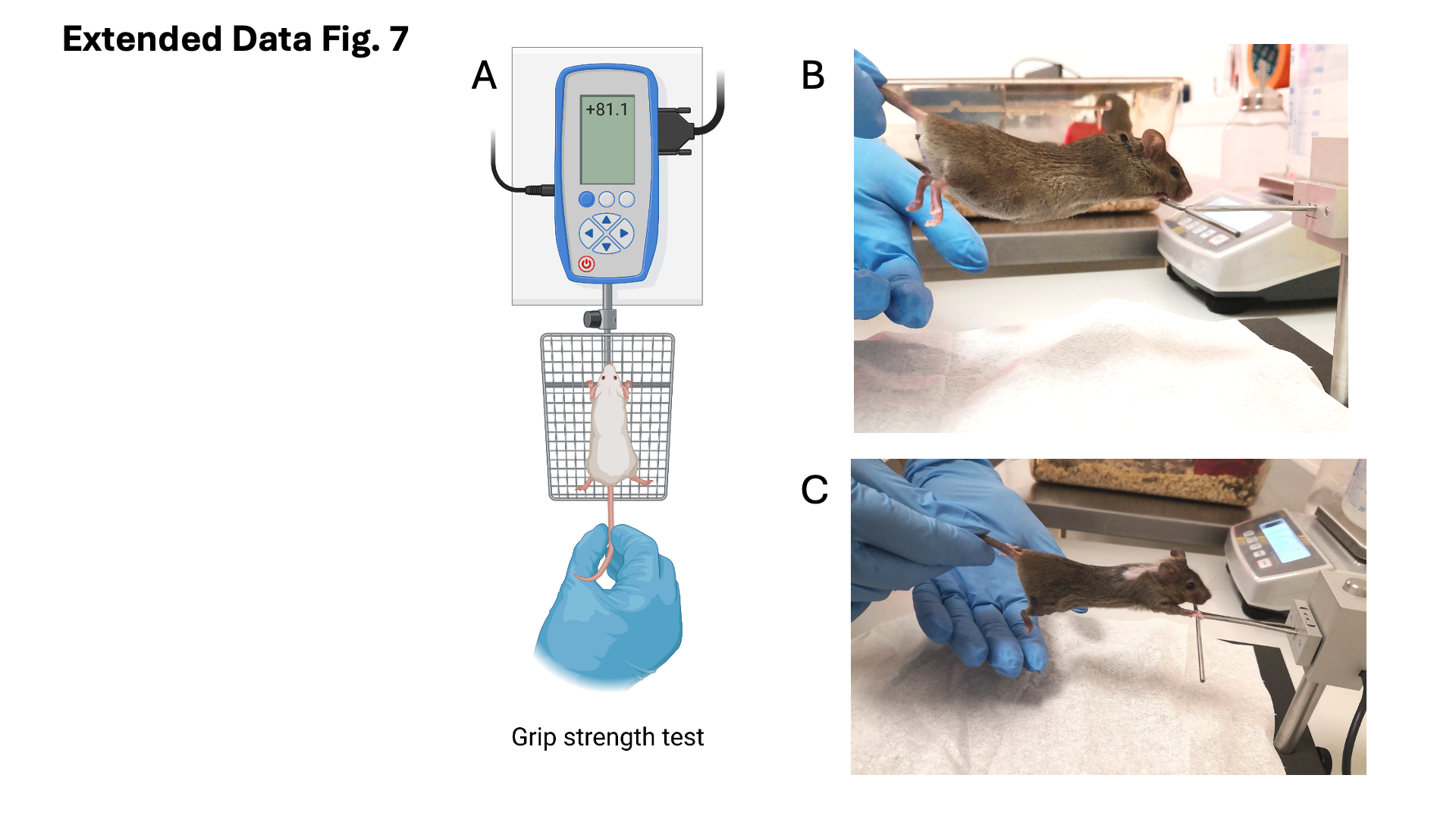
For animals exposed to 11C-ions, the lack of severe toxicity demonstrate that online PET measurement (Fig. 3) correctly predicted the position of the SOBP. However, since the tumor is close to the spine, some activity was inevitably observed in the spinal cord, corresponding to the dose fall-off (Fig. 3). We checked the impact of this residual dose on low-grade toxicity by measuring grip strength performance, a common test to assess cervical spinal injury33 (Extended Data Fig. 7). All results of the bi-weekly grip strength performance for individual mice are reported in Supplementary Fig. 2. A wide inter-individual variability is noted in those curves. However, by pooling the data in Fig. 5A-B we show that the strength of the mice is reduced after irradiation compared to controls, indicative of a minor deficit in neuromuscular function. Correlation of integral PET counts in the spine with individual grip performance is shown in Fig. 5C-D. Despite the wide scatter in the grip test data, there is a significant correlation between activity in the spine and decreased mouse forelimb strength. We therefore clearly demonstrated that the beam online visualization allowed sparing of the OAR and strongly reduced toxicity compared to X-rays.
Washout
The activity in a plastic target decreases after irradiation because of the physical decay of the 11C (T1/2=20.34 min) projectile and nuclear fragments (10C, T1/2=19.3 s; 15O, T1/2=2.04 min). We have previously modelled the radioactive decay with exponential functions that include all fragments produced23. In this experiment, the radioactive decay is overlapped with an unknown biological decay due to the blood flow in the tumor that removes the radioactive isotopes from the site of decay. The degree of vascularization in our tumor model was estimated by perfusion to opacify microvasculature structure in µCT. Supplementary video 3 shows that our osteosarcoma in the neck is highly vascularized, so a strong biological washout is expected. The total washout data for all animals are reported in Supplementary Fig. 3. Studies in Japan in a rat glioma model point to a double-exponential model for the biological washout34, which was also applicable to our data based on the results of the Fisher’s test on fitting parameters. We therefore used the following equation to fit the activity data measured after the irradiation was stopped:
$$\:A\left(t\right)={A}_{phys}\bullet\:{A}_{bio}={A}_{0}{\sum\:}_{i}{w}_{i}{e}^{-\frac{ln2}{{T}_{1/2i}}t}\bullet\:\left[{W}_{s}{e}^{{-k}_{s}t}+(1-{W}_{s}){e}^{{-k}_{f}t}\right]$$
where A0 is the activity at the end of the irradiation, Ws - the relative weight of the slow component, and ks and kf are the slow and fast time constants, respectively. T1/2i is the half-life of the i-th contributing radioisotope and wi is its fraction in the total number of fragments. Based on the FLUKA simulation, we have considered 96% 11C, 3% 10C, and 0.5% 15O ions. Figure 6 shows the pooled analysis of the animals exposed to 5 or 20 Gy (individual curves are reported in Supplementary Fig. 3). The results clearly show a significant difference between the low- and high-dose experiments. The fast component, very well visible at 5 Gy, essentially disappears at 20 Gy. This suggests a quick vascular injury at high doses that delays the washout process in the first half an hour after the irradiation.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}