CASE 1
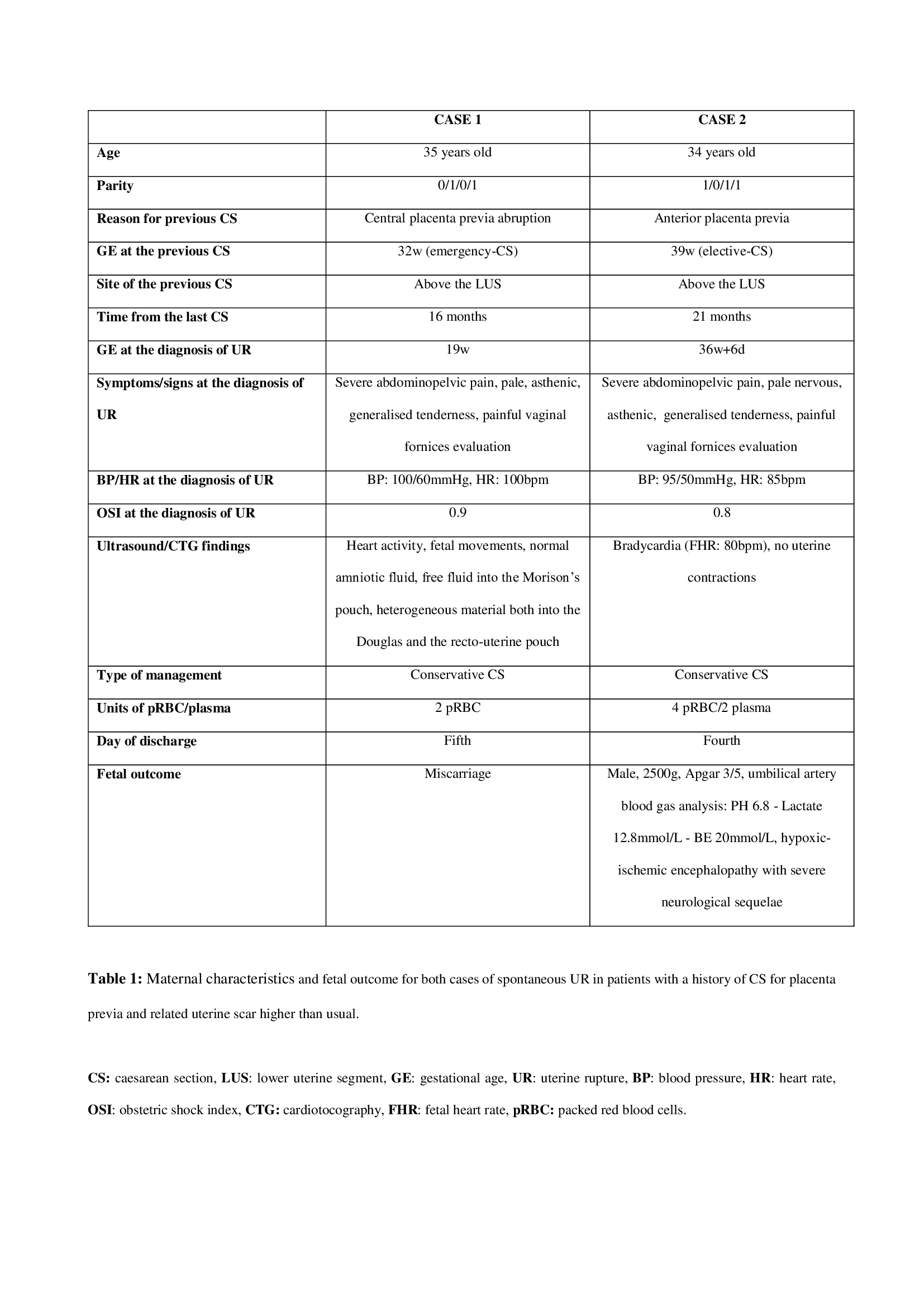
A 35 years old patient with no relevant medical history, parity 0/1/0/1. Her previous pregnancy (December 2017) terminated with an emergency-CS for a central placenta previa abruption at 32 weeks of gestational age (Robson classification group X); a placental flap was extending anteriorly over the LUS for 3 cm and a transverse hysterotomy was performed more cranially than usual. On April 2019 the patient, 19 weeks pregnant, presented to the obstetric emergency unit complaining of a severe abdominopelvic pain: she was conscious, pale and asthenic with BP: 100/60 mmHg, HR: 100 bpm, rhythmic pulse and obstetric shock index (OSI): 0.9 (normal value < 1).
There was evidence of generalised tenderness, but no vaginal bleeding or amniotic fluid leakage; the evaluation of vaginal fornices was very painful, preventing a complete obstetric visit. Both a transvaginal and a transabdominal scan was performed and thus reported: cervical length of 3 cm, single pregnancy, normal heart activity, fetal movements and amniotic fluid level, anterior and normally implanted placenta, free fluid into the Morison’s pouch and heterogeneous material both into the Douglas and the recto-uterine pouch. The hemoperitoneum had an unknown source and it was impossible to exclude an extra-pelvic aetiology; therefore, an emergency-CS with lower midline incision was performed in the presence of a general surgeon. When opening the abdomen, after the drainage of 1000 ml of blood, the diagnosis was immediately clear: the gestational sac was outside the uterus, bulging through a dehiscent hysterotomic breach with sclerotic edges, partially removed and sent for histological examination. (Figure A). After removing the gestational sac and placenta, which was almost totally detached from the uterine wall, the breach was sutured with interrupted stitches and a good haemostasis was obtained, thus supporting the choice of a conservative approach. The haemoglobin level moved from 9.6gr/dL before surgery to 8.5gr/dL after surgery and finally to 7.8gr/dL the first post-operative day: two units of packed red blood cells (pRBC) were administered, together with intravenous iron. The patient was discharged on day fifth, prescribing home therapy with antibiotic, antithrombotic, iron and uterotonic. The histological examination confirmed the presence of scar tissue over the breach edges, the fetus reported no abnormalities and the growth was found to be consistent with the gestational age; placenta was normal as well.
CASE 2
A 34 years old patient with no relevant medical history, parity 1/0/1/1. On September 2017, she had an elective-CS at 39 weeks of gestational age for an anterior placenta previa (Robson classification group V) and, because of that, a transversal hysterotomy was performed above the LUS.
An ultrasound assessment performed during the next pregnancy, at 7 weeks of gestational age, shows the higher CS-scar location (Figure B). On May 2019, pregnant at 36 weeks and 6 days, the patient presented to the obstetric emergency unit after three hours of severe and increasing abdominopelvic pain. From the clinical point of view, she was conscious, nervous, asthenic and pale with BP: 95/50 mmHg, HR: 85 bpm, rhythmic pulse and obstetric shock index (OSI): 0.8 (normal value < 1).
The superficial and deep abdominal palpation revealed a generalised tenderness and the digital evaluation of vaginal fornices was painful, especially when exploring the area close to the pouch of Douglas; the cervix was closed and no vaginal bleeding or amniotic fluid leakage was observed.
A CTG examination pointed out fetal bradycardia (FHR: 80 bpm for 8 minutes) and no uterine contractions; a transabdominal scan could just confirm the fetal bradycardia, without providing any further information. The next step was an emergency-CS with a Pfannenstiel laparotomy over the previous scar. When opening the abdomen and after draining 1500 ml of blood, the fetus was found outside of the uterus; he was immediately extracted and given into the care of neonatologists. The newborn was a male of 2500 g (Apgar 3/5) and the umbilical artery blood gas analysis resulted as follow: PH 6.8 - Lactate 12.8 mmol/L - BE 20 mmol/L. After removing the placenta, almost totally detached from the uterine wall and bulging into the abdomen, a large breach over the middle third of the anterior wall was sutured with interrupted stitches. Obtaining a good haemostasis, a conservative approach was chosen as the best option. Three units of pRBC and two units of plasma were infused during the surgery to balance the huge amount of blood collected into the abdomen and the low haemoglobin level (8.5gr/dL). Straight after the CS, the value was stable (9.5 g/dL) but the following day it decreased to 7.8gr/dL, so requiring another administration of pRBC. The patient was discharged on day fourth, prescribing home therapy with antibiotic, antithrombotic and iron. About the fetal outcome, an MRI performed 30 days after birth diagnosed a hypoxic-ischemic encephalopathy with severe neurological sequelae.
{kind=link}