Participants demographics
Between September 1st to November 30, 2023, a total of 557 responders initiated the survey, and 465 completed all questions, representing around 10% of the urologists in Brazil. All the responses were evaluated and were included at the database. Among them, 370 (69.6%) described themselves as general urologists, 102 (19%) as uro-oncologists and 52 (9.8%) were dedicated to another subspecialty, but also managed uro-oncology patients. Responders not practicing urologic oncology (1.7%) were excluded of the analysis. Seventy per cent of all participants reported not having additional training after residency, but among 102 (19%) uro-oncologists, 75.5% had pursued further education (57.8% fellowship, 28.3% holding master’s degree, 25.5% PhD degree and 14.7% having completed both a fellowship and a PhD degree) (Supplementary files).
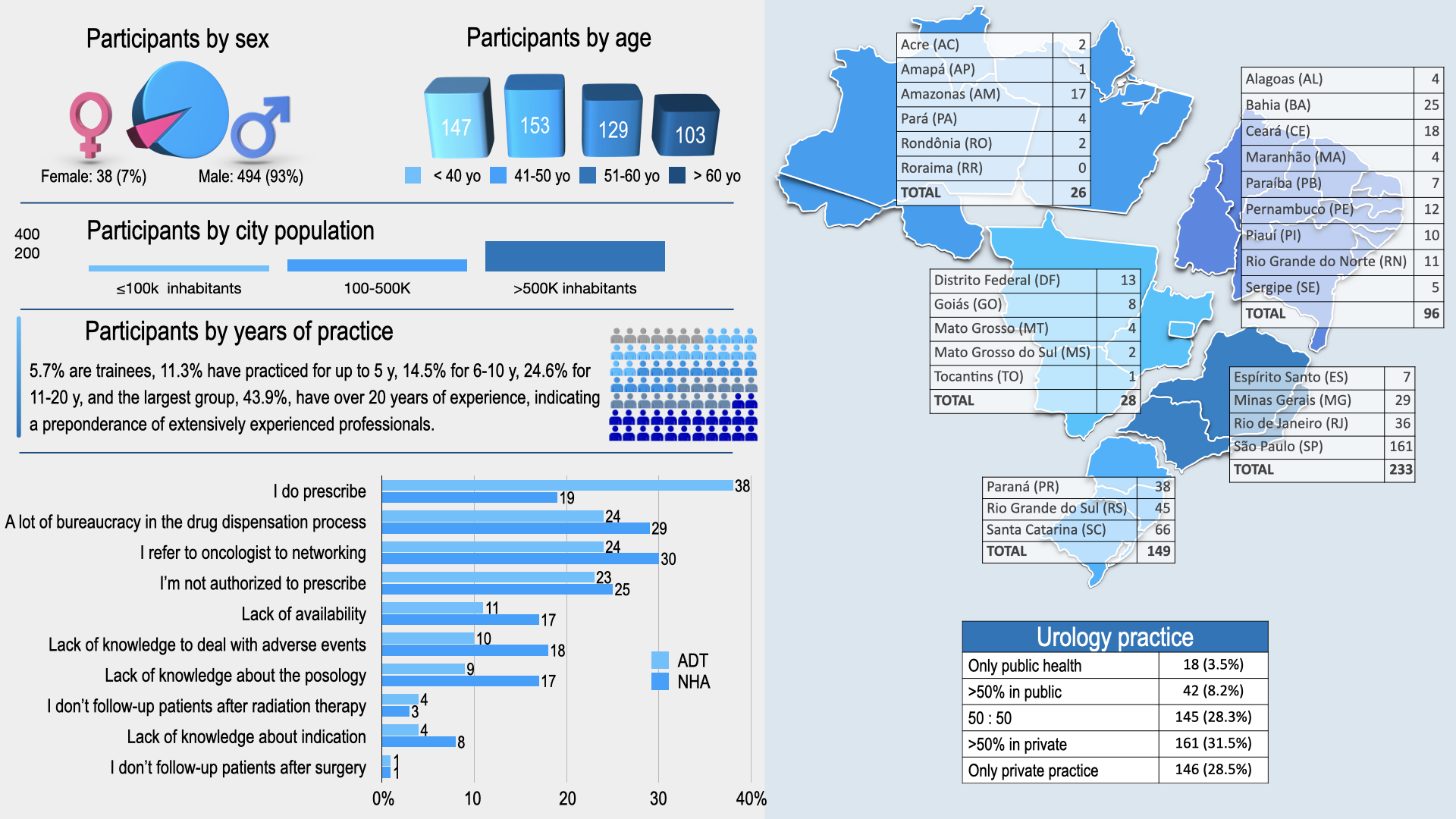
As of 2024, women represent 4% of the urology workforce in Brazil. In this study, 7.2% of the respondents were female urologists. The population characteristics are described on infographics, along with a comparison between global ADT prescribing and new drugs. (Figure 1).
Comparison of the management between different regions of Brazil
The proportion of uro-oncologists varies considerably among regions, with the highest concentration in São Paulo (22.4%) and the lowest in the North (7.7%). There is a predominant male representation among urologists across all regions. The experience of professionals also differs, with the majority having more than 10 years of practice, especially in the Central-West (71.5%) and the Southeast (67.2%) regions.
The majority of survey participants work in both public and private sectors. A minority of urologists are exclusive to only one sector.
During residency, most urologists managed metastatic patients. The use of ARPi was relatively low across all regions, with the highest usage in the Southeast (20.8%) and São Paulo (18.6%).
In current practice, the prescription of LHRHa is most prevalent in São Paulo (47.8%) and the South (38.3%). The prescription of first-generation antiandrogens is most common in the South (42.9%) and less frequent in the Northeast (26%). The prescription of ARPi is highest in the Southeast (27.8%) and São Paulo (23%), but low in the North (7.7%) and Central-West (7.1%). Additionally, urologists who manage more than 2 biochemical recurrence (BCR) patients per month are relatively uncommon, with the highest incidence observed in the Southeast (13.9%) and Central-West (14.3%) regions.
Comparison of the management between general urologist and uro-oncologists
Most of uro-oncologists practice in bigger cities with population >500,000 inhabitants (84.2% vs. 57.2% among general urologists, p<0.001); they attend more oncologic patients per month and are more likely to follow-up the patients after primary treatment for PC (Table 2).
Although 64.7% reported having been trained during residency, merely 41.3% currently prescribe ADT after residency. Notably, 33% of the urologists reported not seeing metastatic patients in everyday practice. On the other hand, despite only 15.3% have been trained to prescribe ARPi, 22.4% currently prescribe ARPi in their practice. Prescription of ADT is higher among uro-oncolgists compared to general urologists: 49.5% prescribe LRRHa (vs. 32.2%) and 43% prescribe ARPi (vs. 17.6%).
When asked about management decision in localized PC setting, 92.7% of the urologists responded that they were responsible for the clinical decision, while 5% of them participate in shared decisions on tumor boards. Also, 97.9% of the participants demonstrated preference to perform radical prostatectomy in this scenario instead of RT (2.2%) and 91.6% of the urologists continue to follow-up the patients after surgery, with no differences between general urologists and uro-oncologists.
When RT is indicated, 88% of the urologists continue to follow-up patients, most of them (61.3%) together with the radiation oncologist and the number is higher among uro-oncologists (95.3% vs. 86.8%, p=0.04). About taking part in the indication of ADT in patients who undergo RT, only 35.5% of the urologists participate on decision making, alone (13.6%) or in conjunction with radiation oncologists (21.9%); and this therapeutic decision rests then with CO (41.7%), radiation oncologist (10.8%) or both (6.5%). Moreover, ADT is most often prescribed by CO (66.2%).
In BCR setting, 58.7% of the participants have PET-PSMA available and 29% use it to re-stage more than half (18.1%) or all (11%) the patients; only 17.6% reported never using it. Also, in this scenario, 90.8% of the urologists continue participating in therapeutic decisions, most of them (57%) together with the CO. And regarding M0 castration-resistant prostate cancer (CRPC) patients, most urologists (63.7%) refer the patient to oncologists for joint decision-making.
ADT pitfalls: Regulatory barriers, access limitations, and pharmacological complexities.
The leading reasons cited for both therapies were remarkably similar, with the bureaucratic complexity of the medication dispensation process being paramount. The percentage of urologists encountering these barriers when prescribing LHRHa ranges from 35.6% in São Paulo to 73.7% in the North. Regarding the prescription of ARPIs, no significant regional variations were observed. Concerns related solely to the clinical use of LHRHa and ARPIs, such as managing side effects and determining appropriate dosages, are less prevalent but still notable. In the Northeast, for example, 47.1% of urologists cited clinical use concerns for LHRHa, the highest among all regions. For ARPIs, these concerns were reported by 17.7% of urologists in the Northeast, with lower percentages in other regions such as São Paulo (7.5%) and the South (7.4%) (Supplementary files).
Specifically, 51.9% of general urologists and 39.5% of uro-oncologists indicated that regulatory and access issues were their primary barriers to prescribing LHRHa. Similarly, both groups faced access and regulatory barriers when prescribing ARPIs. Additionally, 25.3% of general urologists reported concerns related to the clinical use of LHRHa, compared to 15.8% of uro-oncologists. For ARPIs, 63.1% of general urologists and 50% of uro-oncologists expressed similar concerns (Supplementary file).
The prescription rates for LHRHa and ARPIs were notably low, with only 170 urologists (30.5%) prescribing LHRHa and 11 (3%) prescribing ARPIs. Referrals to CO within their professional network were also notable. Specifically, 97 urologists (17.4%) referred patients to oncologists for LHRHa treatment, and 124 urologists (21.2%) did so for ARPi prescriptions (Table 3).
{kind=link}