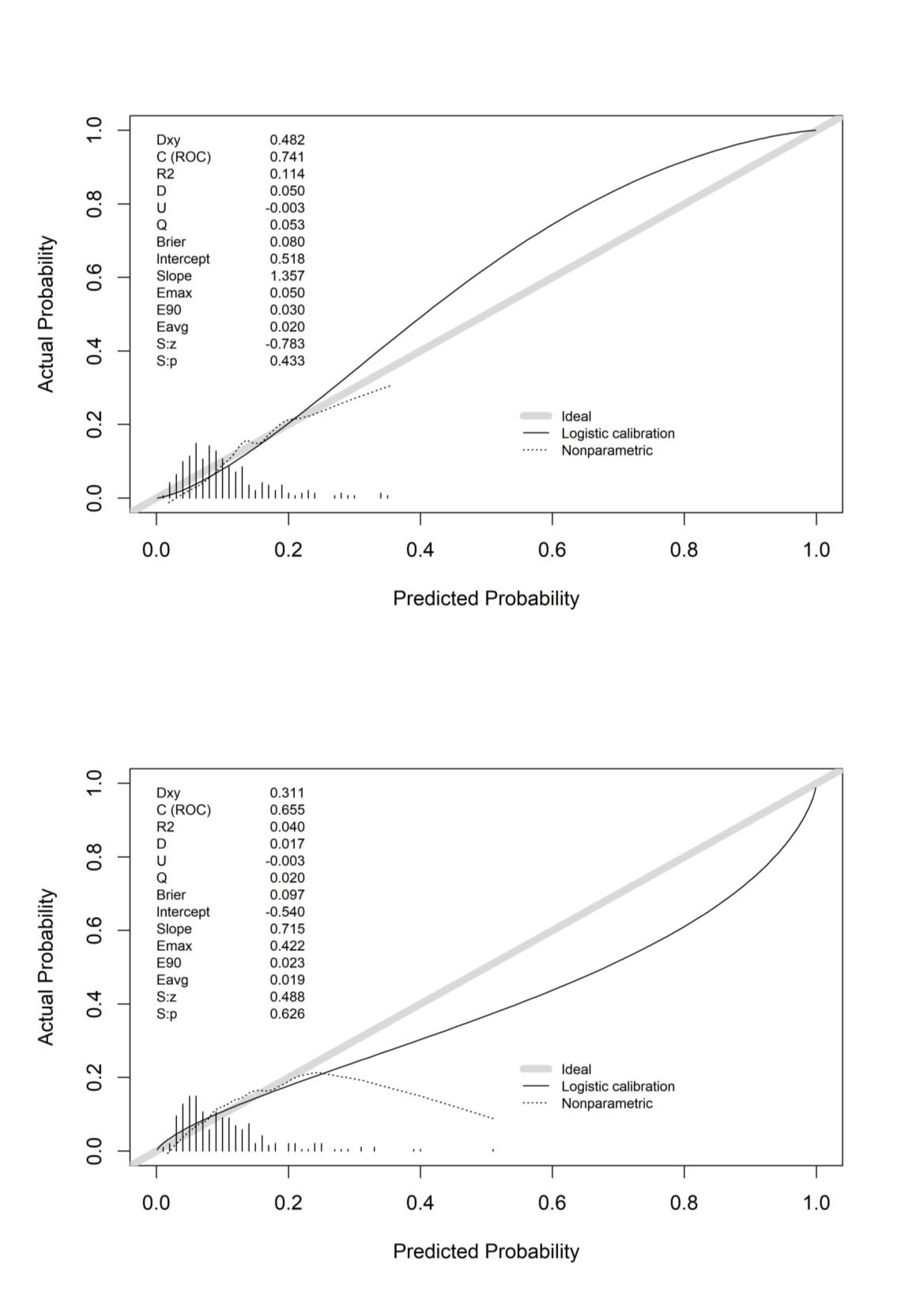
In our study, we enrolled 1,349 patients following elective intracranial surgery, observing a morbidity rate of PS at 10.2%, with 6.3% attributed to hemorrhagic stroke and 4.7% to ischemic stroke. In this study, we developed nine ML prediction models, including LR, GDB, RF, XGBoost, NB, KNN, and DT, was assessed using the test set. Our findings indicate that the LR model excelled in predicting PS, achieving an AUC of 0.741. Furthermore, the LR model exhibited an accuracy rate of 0.668, a sensitivity of 0.650, and a specificity of 0.670.
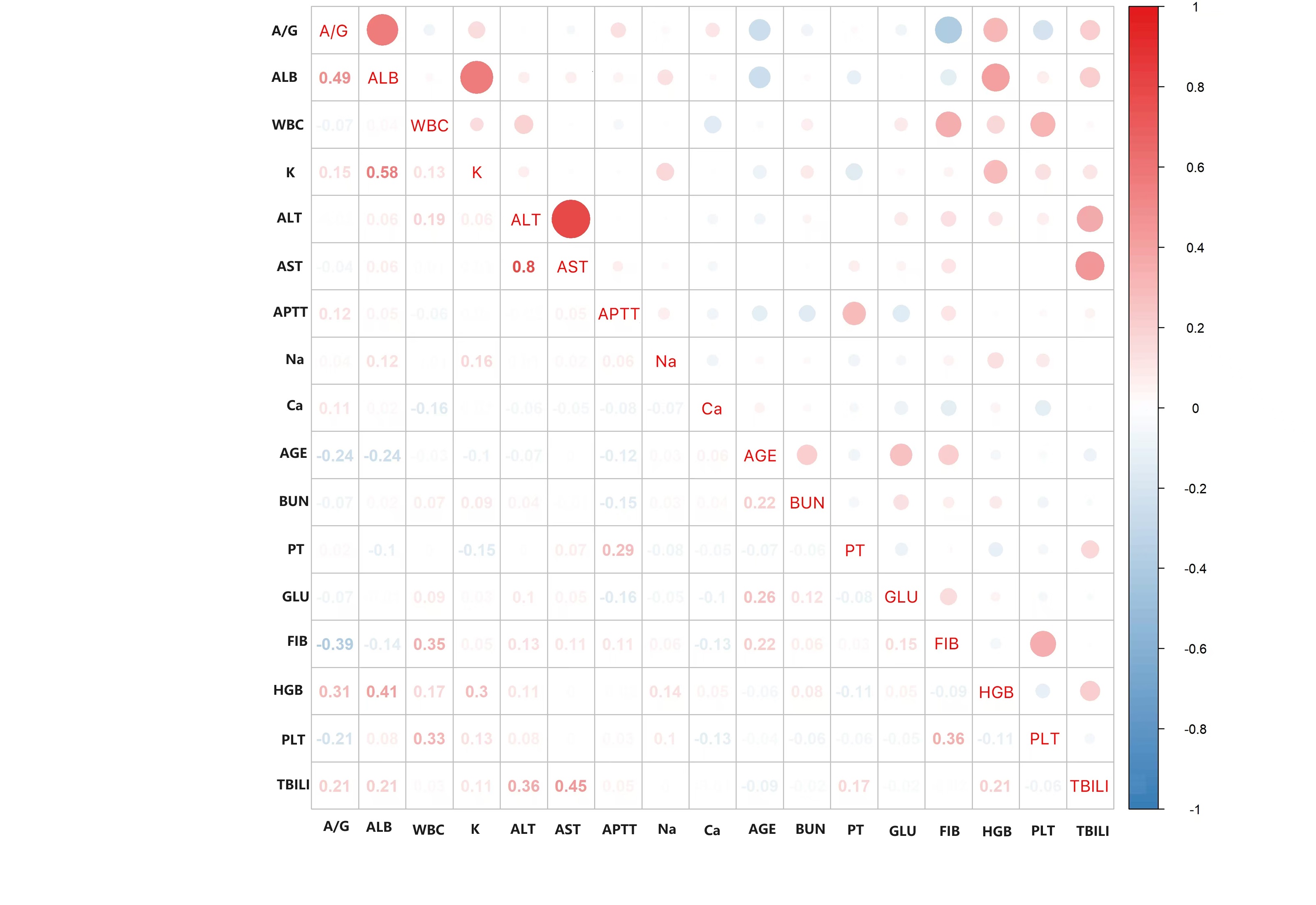
Through feature importance analysis, it was identified that "preoperative plasma albumin level", "ASA classification", "preoperative routine blood hemoglobin level", "plasma albumin/globulin ratio", and "total bilirubin level" emerged as the top five significant features for predicting PS. Most patients with a high ASA classification possess comorbidities, including diabetes mellitus and hypertension, which are recognized risk factors for stroke[25].Several studies have shown that serum albumin levels are significantly and negatively associated with stroke risk[26; 27]. Moreover, long-term mortality is increased in acute ischemic stroke with low or below normal albumin[27]. This correlates with the role of albumin in modulating pyruvate dehydrogenase, which increases the flux of glucose and lactate in astrocytes, enhances the formation of anti-inflammatory lipoxins, resolvins, and protectins derived from docosahexaenoic acid and other polyunsaturated fatty acids, thereby reducing ischemia-induced neuronal damage[28]. Previous studies have consistently demonstrated a correlation between preoperative hemoglobin levels and the incidence and prognosis of PS[29]. Moreover, a meta-analysis provided compelling evidence supporting the association between admission anemia and both ischemic and hemorrhagic stroke, as well as elevated mortality rates related to stroke[30]. The direct link between anaemia and cerebrovascular events is the blood supply, as anaemia results in a reduction of oxygen supply, potentially leading to hypoxic neuronal damage. Moreover, anaemia is considered a hyperkinetic state that disrupts endothelial adhesion molecule genes, which may contribute to thrombus formation[31]. Another contributing factor to the incidence of PS is the preoperative plasma albumin/globulin ratio. In a recent study, Beamer et al. observed that patients presenting with high clinical risk factors for stroke were significantly more likely to experience subsequent vascular events, which were associated with a lower blood albumin/globulin ratio[32]. Wang et al. demonstrated that elevated bilirubin levels are associated with a reduced risk of stroke in adults, which aligns with our results[33]. This finding correlates with the antioxidant, anti-inflammatory, and anti-atherosclerotic properties of serum bilirubin [34; 35].
These indicators mentioned were all incorporated into our prediction model, which typically utilizes data routinely collected after admission, underscoring the model's practical feasibility and generalizability within a hospital setting. The predictive factors identified in our model align with the risk factors highlighted in several prior studies, reinforcing its validity. The LR algorithm employed in this study offers distinct advantages over traditional statistical methods, including a transparent model structure and a probability derivation that is robust and open to scrutiny. The parameters within the model elucidate the impact of each feature on the outcome, providing high interpretability. Moreover, the model supports online learning, enabling easy parameter updates without the need for retraining the entire model. Consequently, this model not only integrates the predictive efficiency of key factors but boasts commendable interpretability.
Currently, there is a paucity of research on PS in the field of neuroanesthesiology[36]. Nonetheless, among the sparse ML studies available, one conducted by Zhang et al. stands out[11]. They discovered that the XGBoost model displayed the highest AUC of 0.78 for predicting PS in elderly patients. The study identified hypertension, cancer, congestive heart failure, chronic lung disease, and peripheral vascular disease as the top five predictors[11]. It is important to highlight that the study did not place any restrictions on the types of surgical procedures evaluated, potentially encompassing high-risk interventions for stroke, such as cardiac macrovascular surgery. Additionally, another study identified advanced age, pre-existing valvular heart disease, previous stroke, emergency surgery, and postoperative hypotension as independent risk factors for PS[37]. Patients necessitating emergency surgery exhibit a heightened vulnerability to postoperative complications, including postoperative seizures. Consequently, these patients were excluded from the aforementioned studies to ensure a more focused and controlled analysis of risk factors and outcomes.
The incidence of PS can be linked to a variety of pathologic and physiologic mechanisms. The administration of anesthesia and the execution of the surgical procedure provoke a systemic inflammatory response, leading to alterations in the concentrations of inflammatory mediators and the coagulation status of the blood. These alterations enhance the risk of perioperative thrombosis and intravascular plaque instability, subsequently elevating the probability of stroke in perioperative patients [38; 39].
Our research represents the inaugural effort to construct a predictive model for PS using a ML-based LR algorithm, specifically designed for patients undergoing elective intracranial surgery. This model is distinguished by its explainability through feature importance analysis. Moreover, by statistically addressing the issue of unbalanced data, we have developed a practical predictive tool that enables clinicians to fine-tune clinical therapy.
Nonetheless, our study is not without its limitations. Firstly, the presence of missing values in the original dataset could compromise the stability of our predictive ML model. Secondly, the study's sample size was relatively small, necessitating a larger, multicenter sample to further substantiate the predictive model's validity. Thirdly, this predictive model requires an independent dataset to assess its extrapolation and generalization capabilities accurately. The accuracy of our final model is limited by the relative inadequacy of included data items and the complexity of PS. Lastly, anesthesia-related incidents such as persistent intraoperative hypotension/hypertension during the perianesthetic period were not included due to insufficient data availability. Future endeavors will focus on gathering comprehensive external validation datasets to enhance the validity of this model.
{kind=link}
{kind=link}