The main findings of the present study were: i) ICU and hospital mortality were 32% and 39% for the entire cohort of patients admitted to the ICU and for those who received invasive mechanical ventilation, respectively; ii) 28-day mortality was 24% and 29% for the whole group of patients admitted in the ICU and for those who required invasive mechanical ventilation, respectively; iii) patients who eventually died had already increased risk of death even on ICU admission, as suggested by the high values of APACHE II and SOFA scores, the presence of current malignancy and occurrence of cardiac arrest, and general need for circulatory support with noradrenaline; iv) the primary cause of death of all patients was multi-organ failure most commonly due to sepsis, whereas none died from refractory hypoxemia, neurologic dysfunction or withdrawal of life support; and v) hospital stay was long in patients who survived, frequently complicated by bacteremias.
ICU and hospital mortality of 32% for overall ICU admissions observed in the present study was similar to that recently reported by Auld et al (10) in a large cohort of critically ill patients (n = 217) admitted in COVID-designated ICUs of 3 hospitals in Atlanta, Georgia, showing 28.6% ICU mortality and 31% hospital mortality. Moreover, ICU and hospital mortality of 39% for the approximately four-fifths of patients in our cohort who received invasive mechanical ventilation was also similar to that of Auld et al (10), reporting 33.9% ICU mortality and 35.7% hospital mortality. Notably, only 2.4% of patients in our cohort and 4.8% of patients in the previous study (10) still remained on the ventilator at the time of the report, and there was ample follow-up time (median 50 days, range 29–88 days, in our group of patients) (Table 2). Both patient cohorts, i.e., that of ours and that of Auld et al (10), seem comparable in terms of lung disease and patient illness severity, at least on ICU admission. Indeed, median PaO2/FiO2 was 121 mmHg (IQR, 86–171 mmHg) with median PEEP 14 cmH2O (IQR, 12–16 cmH2O) in our cohort versus median PaO2/FiO2 of 132 mmHg (IQR, 100–178 mmHg) (PEEP level was not reported) in the previous study (10); median SOFA score was 7 in both studies. Most of our patients had moderate and severe ARDS according to the ARDS Berlin Definition (14); the definition of ARDS was also fulfilled in most of our mechanically ventilated patients on the day of intubation, as the median Lung Injury Score was 2.7 (IQR, 2.5–3.2) (17) (Table 1). Our data, as well as that of Auld et al (10), provide evidence that mortality rates of severely ill COVID-19 patients with ARDS may be comparable or even lower to those reported in ARDS of different etiologies (19, 20) including Influenza A (21, 22). Indeed, hospital mortality for patients with moderate ARDS was 40.3% and for those with severe ARDS was 46.1% (19), whereas overall pooled mortality rate of all ARDS studies included in a comprehensive literature review was 43% (20). Moreover, mortality rate was 41.4% (21) and 46% (22) among ICU patients with Influenza A pneumonia, most of whom had ARDS.
Our findings differ from those of earlier studies in ICU patients with COVID-19 reporting overall mortality rates 49–62% (2, 7, 8) and mortality rates as high as 66–97% among patients requiring invasive mechanical ventilation in China (7, 23, 24). Similarly, mortality rate for our patients was substantially lower than that of subsequent reports from USA (4–6), showing mortality rates for patients requiring invasive mechanical ventilation ranging from 52% (5) and 67% (6) in the Seattle region to 88.1% in New York area (4), as well as from Italy demonstrating overall hospital mortality 53.4% for patients admitted in ICU (25). To interpret the observed differences in clinical outcomes, at least two general and/or local factors should be taken into account. Firstly and primarily, in our study all critically ill patients with COVID-19 were admitted to the ICU in time, because overwhelming stress on the healthcare system did not occur in our country (11). All these patients were admitted to preexisting multidisciplinary ICUs, were cared for by critical care teams with experience in the management of patients with severe acute respiratory failure at standard staffing ratios, and received full intensive care support, including renal replacement therapy. Secondly, the onset and peak of the COVID-19 pandemic in Greece occurred later than in many of the regions from earlier reports, including neighboring Italy (25). This delay gave time to create organizational arrangements, purchase equipment, train personnel, make consensus-driven clinical protocols, and distribute supplies across the healthcare system.
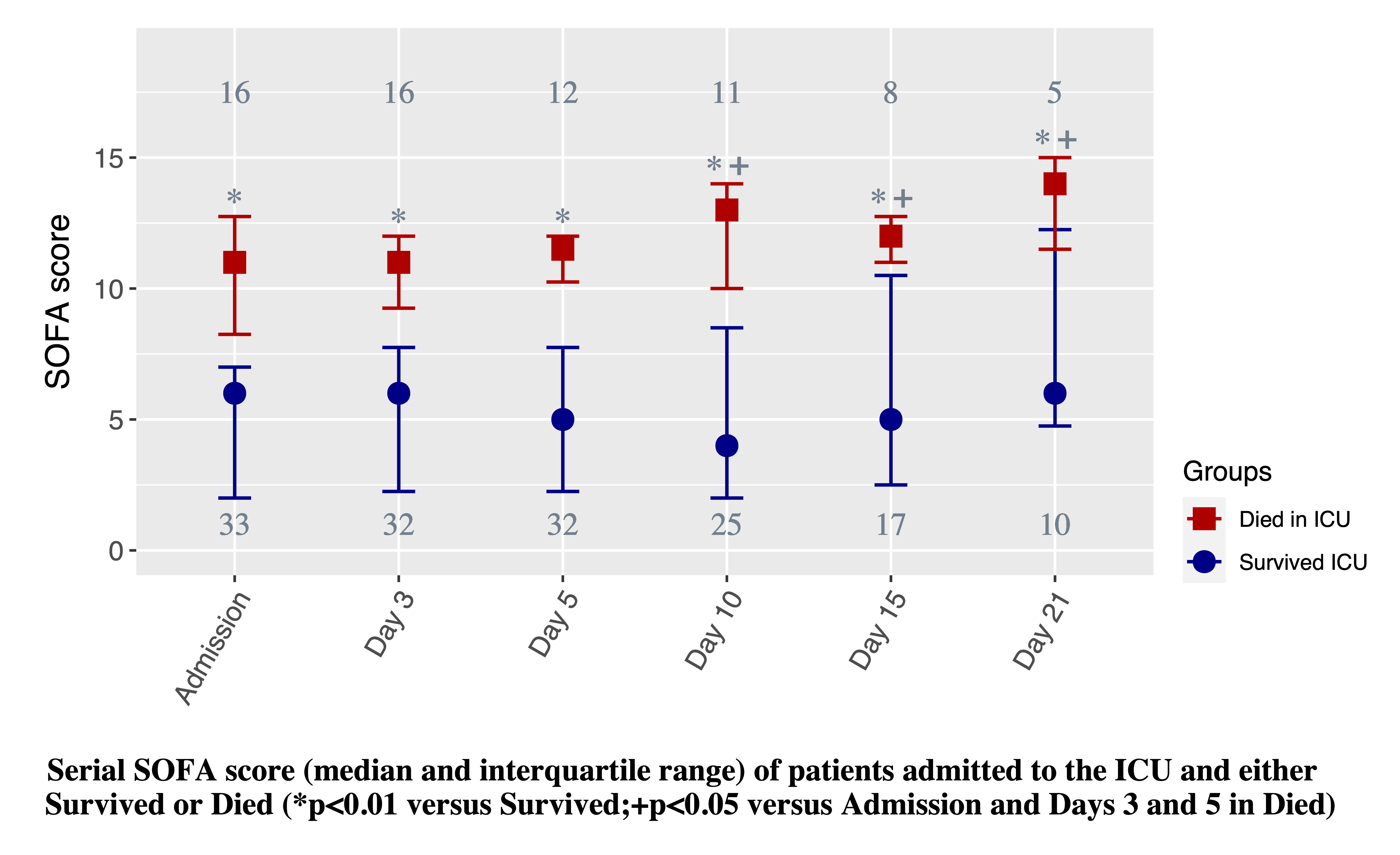
Lung disease on ICU admission was not worse in patients who died than in those who survived as suggested by lack of any difference in blood oxygenation, respiratory system compliance and Lung Injury Score values; the same ventilatory protocol was also applied in both groups as implied by the presence of no difference in PEEP, plateau pressure and driving pressure levels (Table 1). Moreover, lung disease severity on admission and ICU days 3–21 did not contribute to the higher SOFA score in patients who died compared to those who survived (Fig. 2) and nobody died from refractory hypoxemia. The higher SOFA score on admission and ICU days 3–21 (Fig. 2) was mainly due to higher cardiovascular and renal components of SOFA score. Not surprisingly, patients who died compared to patients who survived, more commonly needed noradrenaline infusion for circulatory support on ICU admission (Table 1) and required noradrenaline use for shock treatment and continuous renal replacement therapy for renal failure management during ICU stay (Table 2).
We acknowledge the main limitation of this study, i.e., we reported findings and outcomes from a single center and included a rather limited number of patients compared to hundreds or thousands of patients incorporated in many studies from other countries with thousands victims of COVID-19 pandemic (2–4, 9, 23, 25, 26). However, our study included all consecutive patients admitted to four COVID-designated ICUs of the biggest referral center for COVID-19 in Greece and our study sample represents about 25% of the total number of patients admitted in Greek ICUs (27). Due to the relatively limited spread of the pandemic in Greece, our medical system was not overwhelmed, and this fact generated the purpose of the present study. Therefore, our findings might not be generalizable to different populations and medical systems, but might be relevant to other countries where the pandemic did not overwhelm the health system capacity.
{kind=link}