2.1 Study participants
The study encompassed a population of adolescents with depression, and the sample comprised adolescents diagnosed with depression and treated at Nantong Fourth People's Hospital, Nanjing Brain Hospital, and Suzhou Guangji Hospital from December 2022 to July 2023. Inclusion criteria: ① age range of 11–18 years[10]; ② fulfillment of the diagnostic criteria for depression (experiencing a persistently depressed mood or reduced interest in activities for at least two weeks, accompanied by difficulty in concentrating, feelings of worthlessness, or excessive and inappropriate guilt and self-guilt, hopelessness, etc.) as outlined in the ICD-11 Classification of Mental and Behavioral Disorders: Clinical Description and Diagnostic Points[11]; ③ possession of adequate communication skills, including the ability to read and express oneself accurately. Exclusion criteria: ① individuals diagnosed with other mental disorders; ② those with a history of alcohol and drug abuse; ③ presence of severe physical illnesses; ④ abnormalities in hearing or vision; ⑤ suicidal behaviors (jumping from heights, hanging, ingesting lethal doses of drugs, and other obvious suicidal and self-injurious behaviors for death).
2.2 Sample size
The model construction was based on the minimum of observations for both types of outcomes in the dichotomous outcome. The literature indicates a prevalence of 51% for NSSI among adolescents with depression. Given the inclusion of 10 model variables, the final sample size requirement was assumed to be 205 cases(minimum of 100), adhering to the ten events per variable (EPV) principle. Considering a 10% missing rate, invalid questionnaires, and a substantial number of missing values, 228 cases were included for the training set and internal validation, with 70% allocated to the training set and 30% for internal validation. External verification consisted of the same sample size as the internal validation, requiring an additional 68 cases. Therefore, the total planned sample size for this study was 296 cases. Ultimately, 596 patients were included.
2.3 Methods
2. 3.1 General information survey
A self-administered questionnaire was utilized to collect data on age, sex, whether there is self-injury, being a single child, relationships and love experiences, sleep duration, online activity duration, parental education, cohabitation status, parental marital status, parental relationships, residence, and family income.
2.3.2 The Eysenck personality questionnaire (EPQ): It was initially developed by Donald E[12], and subsequently sinicized and revised by Gong Y.X[13]. It was employed to assess the personality dimensions of the patients. The questionnaire consists of 88 questions and includes three personality subscales: extraversion (E), neuroticism (N), and psychoticism (P), and a validity subscale (L). The cumulative scores of each subscale were transformed into standardized T-scores based on age and gender norms.The Cronbach's α-coefficient is 0.81.
2.3.3 The Family Intimacy and Adaptability Scale (Family Adaptation and Cohesion Evaluation Scales II, FACES II): It was developed by Olson in 1982[14], and subsequently sinicized and revised by Fei L.P[15]. It encompasses two subscales: 'Family Intimacy' (the emotional interconnectedness of individual family members) and 'Family Adaptability' (the capacity of individual members to make appropriate adjustments in response to varying family dynamics and stages). FACES II is a tool for evaluating family functioning by measuring intimacy and adaptability. The scale demonstrated satisfactory reliability and validity, with Cronbach's α-coefficient of 0.85. 2.3.4 Self-esteem scale (Rosenberg self—esteem scale, SES): It was initially developed by Rosenberg M[16], and later sinicized and revised by Ji C.F[17].This scale examines an individual's positive or negative self-attitude. Comprising ten questions graded on a four-level scale from "very consistent" to "very inconsistent," the ranking reflects the level of self-esteem, with higher scores indicating elevated self-esteem. The scale's robust internal consistency is characterized by Cronbach's α-coefficient of 0.90.
2.3.5 Conner–Davidson Resilience Scale (CD-RISC10): CD-RISC10 was derived from the work of Campbell-Sills and Stein[18], later sinicized and revised by Dai X.Y[19]. It serves as a concise iteration of the CD-RISC, gauging an individual's resilience and adaptive capacity when confronted with adversity. The scale, involving ten self-rated items, employs a 5-point Likert scale from 0 ("not true at all") to 4 ("true nearly all the time"). The resulting scores, ranging from 5 to 50, correlate with higher levels of resilience. The CD-RISC10 exhibits robust internal reliability (Cronbach's α = 0.89).
2.3.6 Childhood trauma questionnaire (CTQ): A simplified adaptation of the CTQ, initially revised by Bernstein et al[20]. and later by Zhao. X.F[21]. in 2003 assesses the abuse and neglect experienced during childhood. The CTQ comprises 28 items categorized into five subscales: emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. The Cronbach's α-coefficient is 0.82.
2.3.7. Adolescent Social Support Scale(Social support rate scale, SSRS): According to Xiao.'s social support theory[22], Yei and Dai compiled a social support scale for adolescents in 2008[23].This scale comprises three dimensions: subjective social support, objective social support, and utilization of social support. These dimensions evaluate the social support available to adolescents and their interaction with this support system. The scale encompasses 17 items, each rated on a five-point scale, with "Meets" receiving 5 points, "Somewhat Meets" = 4 points, "Unsure" = 3 points, "Somewhat" = 2 points, and "Not sure" = 1 point. The scale's internal consistency, Cronbach's α-coefficient is 0.82.
2.3.8 Adolescent Society Life Events Scale (ASLEC): Compiled by Liu[23], this scale assesses the frequency and intensity of stressful life events among adolescents, particularly middle school and college students. The correlation coefficients between individual event scores and the total score range from 0.24 to 0.57, averaging 0.45. This scale demonstrates satisfactory reliability and validity, with Cronbach's α-coefficient of 0.85.
2.3.9 Barratt Impulsivity Scale (BIS-11) The 11th edition of the Impulsivity Scale was compiled by Barratt et al. and revised by Zhou L. et al[24]. was used to assess the impulsivity trait, which has a Cronbach's α-coefficient of 0.76, retest reliability of 0.85, and a good structural validity index. The questionnaire consists of 26 items covering three dimensions, namely attentional impulsivity, locomotor impulsivity and unplanned impulsivity, and is scored on a 4-point scale (from 1 'never' to 4 'all the time'), with higher scores indicating greater impulsivity.
2.3.10 Self-Rating Anxiety Scale (SAS) SAS was derived from the work of Zung W.W[25]. It is a unidimensional scale with 20 items, including five reverse-scored questions. The sum of the scores for each item was multiplied by 1.25 and rounded to the nearest whole number to obtain the standardized anxiety score. A 4-point Likert scale was used, with one indicating none or very little time, four indicating most or all of the time, and four indicating most or all of the time. The total standardized score ranges from 25 to 100, with higher scores indicating greater levels of anxiety. Higher scores indicate greater levels of anxiety. The scale has a cut-off for anxiety, with < 50 indicating no anxiety, 50–59 indicating mild anxiety, 60 − 59 indicating moderate anxiety, and ≥ 70 indicating severe anxiety. The Cronbach's α-coefficient is 0.86.
2.3.11 Self-Rating Depression Scale (SDS) The scale was developed by Zung to quantify the amount of money received. Measure the severity and treatment of depressive state Changes in therapy(zung 1971). There are 20 items on the scale. Using a 4-level scoring method, each of the 20 items. If you add up all the scores, you get a rough score; Multiply by the rough parts. Take the integer part after 1.25. Obtained standard Points. The higher the standard score, the more severe the depression. According to the results of the Chinese norm, the SDS standard is divided into 53 points, 53 to 62 points for mild depression, 63 to 72 was classified as moderate depression, and ≥ 72 was classified as severe depression. The Cronbach's α-coefficient is 0.86.
2.4. Statistical analysis
2.4.1 Analytical methods
Two individuals entered all survey data into Excel software. There were four missing data concerning parental relationships, one regarding parental mental health, six related to family income, and six others regarding delivery mode. Data with less than 5% missing values required no filling. Statistical analysis was conducted using SPSS 25.0 and R language 4.1.1. Normally distributed measurement data in two samples were represented by mean and standard deviation and compared using an unpaired two-tailed t-test. Count data variables were expressed as frequencies and percentages, with comparisons made using the χ2 or Fisher's exact tests.Significant.Statistical significance was set at P < 0.05.
2.4.2 Variable selection and prediction model establishment
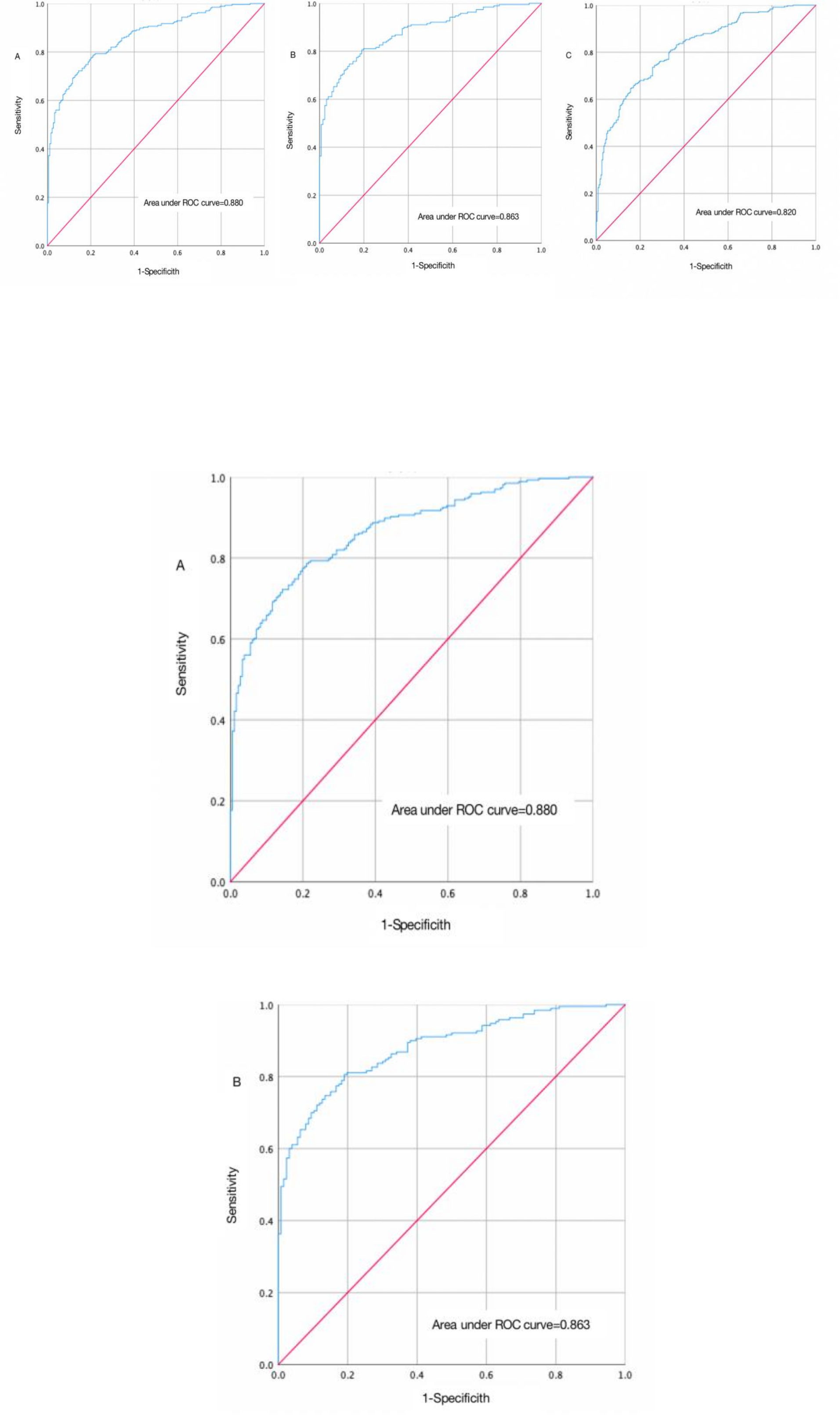
Initial screening of variables was performed using single-factor analysis. Subsequently, LASSO regression was employed to identify predictive factors. Factors selected from the LASSO regression were then incorporated into binary logistic regression for further analysis. Only those factors demonstrating statistical significance (P < 0.05) were retained for inclusion in the risk prediction model.The dataset was randomly partitioned into training and validation sets, with 70% allocated for model development. The performance of the risk prediction model was evaluated using the following metrics. The Area Under the Curve (AUC) was computed to assess the model's discriminatory ability in distinguishing between different outcomes. Calibration curves of the ROC were also generated to assess model calibration.This test was employed to evaluate the goodness-of-fit of the model.Decision Curve Analysis (DCA) was utilized to assess the clinical utility of the risk prediction model across various threshold probabilities.
2.4.3 Internal and external validation of the model
30% of the information was used for internal validation of the risk prediction model, and data from other hospitals were conveniently extracted for external validation, and the area under the ROC curve, AUC, Hosmer-Lemeshow goodness-of-fit test, calibration curve, and DCA were used to evaluate the discriminability, calibration and clinical utility of the NSSI prediction model, respectively.
2.5 Data collection
①Setting and Participant Selection: Data collection was conducted in two distinct settings: outpatient and ward environments. For outpatient data collection, patients were selected based on their preference for a quiet, comfortable, and well-lit single-room clinic environment following consultation. In the ward setting, patients were chosen based on their stable mood and preference for a quiet, comfortable, and private meeting room.②Participant Recruitment and Consent༚Adolescent patients diagnosed with depression were recruited for this study. Prior to participation, detailed explanations regarding the study's purpose, content, and significance were provided to both the adolescent patients and their parents or legal guardians. Informed consent was obtained from all participants, and assent was secured from adolescent patients. A signed informed notification letter was provided, outlining the study's scope and providing guidance for completing the questionnaire.③Questionnaire Administration༚A standardized approach using uniform instructions and terminology was employed to guide adolescent patients with depression through the questionnaire assessment process. Additional explanations and clarifications were offered to participants to address any queries or uncertainties they may have had during the completion of the questionnaire.
2.6 Ethical considerations
This paper adheres to the ethical principles set forth in the Declaration of Helsinki by the World Medical Association. The ethical considerations guiding this study encompass:
2.6.1 Informed Consent: Prior to participation, all subjects provided informed consent. They were informed comprehensively about the study's objectives, procedures, potential risks, and their right to withdraw at any time without repercussion.
2.6.2 Confidentiality: Strict measures were implemented to safeguard participant confidentiality. All data collected were anonymized and securely stored to prevent unauthorized access.
2.6.3Beneficence and Non-maleficence: The study aimed to maximize benefits for participants while minimizing potential harm. Stringent measures were taken to mitigate risks during data collection and analysis.
2.6.4 Research Design and Approval: The study was approved by the Ethics Committee of the Fourth People’s Hospital of Nantong City (approval no.: 2022-Ko37)
2.6.5Conflict of Interest Disclosure: The researchers affirm no conflicts of interest that could have influenced the study's outcomes or interpretations.
2.6.6 Participant Treatment: Participants were treated with utmost respect and dignity throughout the study. Their voluntary participation was paramount, and efforts were made to ensure their comfort and safety.
2.6.7 Regulatory Compliance: This study adhered to all relevant laws and regulations governing research involving human subjects in China.
{kind=link}