Study design and participants
The CoLaus|PsyCoLaus study is a population-based study investigating the epidemiology and genetic determinants of psychiatric and cardiovascular disease in Lausanne, Switzerland (16). Briefly, a representative sample was collected through a simple, non-stratified random sampling of 19,830 individuals (35% of the source population) aged between 35 and 75. The baseline study was conducted between June 2003 and May 2006; the first follow-up was performed between April 2009 and September 2012.
In each survey, participants attended the survey unit in the morning after an 8-h fast. Participants answered questionnaires, underwent a clinical examination, and had their blood collected. Blood samples were drawn for analyses and additional aliquots were stored at − 80°C for BCAA analysis. For this study, data from the first follow-up was considered.
Dietary intake, dietary scores and compliance to dietary recommendations
Dietary intake was assessed using a self-administered, semi-quantitative food frequency questionnaire (FFQ) which also included portion size (17). This FFQ has been validated in the Geneva population (17, 18). Briefly, this FFQ assesses the dietary intake of the previous 4 weeks and consists of 97 different food items that account for more than 90% of the intake of calories, proteins, fat, carbohydrates, alcohol, cholesterol, vitamin D and retinol, and 85% of fibre, carotene and iron. For each item, consumption frequencies ranging from “less than once during the last 4 weeks” to “2 or more times per day” were provided, and the participants indicated the average serving size (smaller, equal or bigger) compared to a reference size. Each participant brought along her/his filled-in FFQ, which was checked for completion by trained interviewers the day of the visit.
For this analysis, we used all 91 items available on the FFQ, together with 16 macronutrients and some micronutrients extracted from it. We also grouped the different food items into categories, i.e., dairy, meat, processed meat, fish, vegetables, and fruits.
Four dietary scores were computed based on the Mediterranean diet. The first Mediterranean dietary score (designated as ‘Mediterranean score 1’) was derived from Trichopoulou et al(19). The score uses consumption frequencies instead of amounts. Briefly, a value of 0 or 1 is assigned to each of seven foods using their gender-specific medians as cut-off. Participants whose consumption frequencies for “healthy” foods (vegetables, fruits, fish, and cereal) were above the median were given the value of 1, while for “unhealthy” foods (meat, dairy products), consumption frequencies below the median were given the value of 1. Two other items were considered: ratio of monounsaturated to saturated fats and moderate alcohol consumption (between 5 and 25 g/day for women and 10 and 50 g/day for men). The score ranges between 0 and 8. The second Mediterranean dietary score (designated as ‘Mediterranean score 2’) adapted to the Swiss population was computed according to Vormund et al (20). It used the same scoring system but considered nine types of “healthy” foods: fruits, vegetables, fish, cereal, salads, poultry, dairy products and wine. The score ranges between 0 and 9. For both scores, higher values represented a healthier diet.
Participants were also dichotomized according to whether they followed the dietary recommendations for fruits, vegetables, meat, fish and dairy products from the Swiss Society of Nutrition (21, 22). Compliance was estimated from the FFQ data. The recommendations were ≥ 2 fruit portions/day; ≥3 vegetable portions/day; ≤5 meat portions/week; ≥1 fish portion/week and ≥ 3 dairy products portions/day. In this study, we did not use portion size to compute compliance, but relied on consumption frequencies. This was done as the portion sizes recommended by the Swiss Society of Nutrition do not take into account a subject’s corpulence and caloric needs (23). As the FFQ queried about fresh and fried fish, two categories of compliance to fish consumption were considered: one included and one excluded fried fish. For each participant, the number of guidelines complied to was computed. Two sums were computed: one used compliance to fish consumption using all types of fish preparation (i.e., including fried fish); the other used compliance to fish consumption using fresh fish only.
Sample preparation and metabolic profiling
Absolute quantification of BCAA was performed by extracting 20 µL of fasting serum samples with 250 µL of ice-cold methanol, adding the internal standard solution of the corresponding BCAA, and diluting it to 300 µL with 0.1% formic acid in water. After the samples were mixed evenly by shaking, they were centrifuged at 4°C and 2700g for 15 minutes. The resulting supernatant was transferred to LC-MS vials prior to injection. A detailed description of the method used has been published(24). Briefly, a hydrophilic interaction chromatography (HILIC)-based high-resolution mass spectrometry (HRMS) was developed, taking advantage of HRMS data acquired in full-scan mode. Accuracy was within 90–106% of validated NIST reference plasma concentrations for the panel of measured BCAA. BCAA extraction recoveries were 87–100% on average, depending on the concentration range spiked. The coefficient of variation (CV) was 1–10% and 1–25% for intra- and interday measurements, respectively.
Other covariates
Smoking status was self-reported and categorized as never, former, and current. Marital status was categorized as living alone (i.e., single, divorced or widowed) or living with a partner. Education was categorized into low (compulsory + apprenticeship), medium (high school) or high (university level). Nationality was dichotomized into born in Switzerland or elsewhere. Presence of any type of diet (i.e., for slimming, diabetes, or hypertension) was also collected and categorized as present/absent.
Physical activity was assessed by a questionnaire validated in the population of Geneva(25). This self-reported questionnaire assesses the type and duration of 70 kinds of (non)professional activities and sports during the previous week. Sedentary status was defined as spending over 90% of the daily energy in activities below moderate- and high-intensity (defined as requiring at least 4 times the basal metabolic rate(26)).
Body weight and height were measured with participants barefoot and in light indoor clothes. Body weight was measured in kilograms to the nearest 100 g using a Seca® scale (Hamburg, Germany). Height was measured to the nearest 5 mm using a Seca® (Hamburg, Germany) height gauge. Body mass index (BMI) was computed and categorized into normal (BMI < 25 kg/m2), overweight (25 ≤ BMI < 30 kg/m2) and obese (BMI ≥ 30 kg/m2).
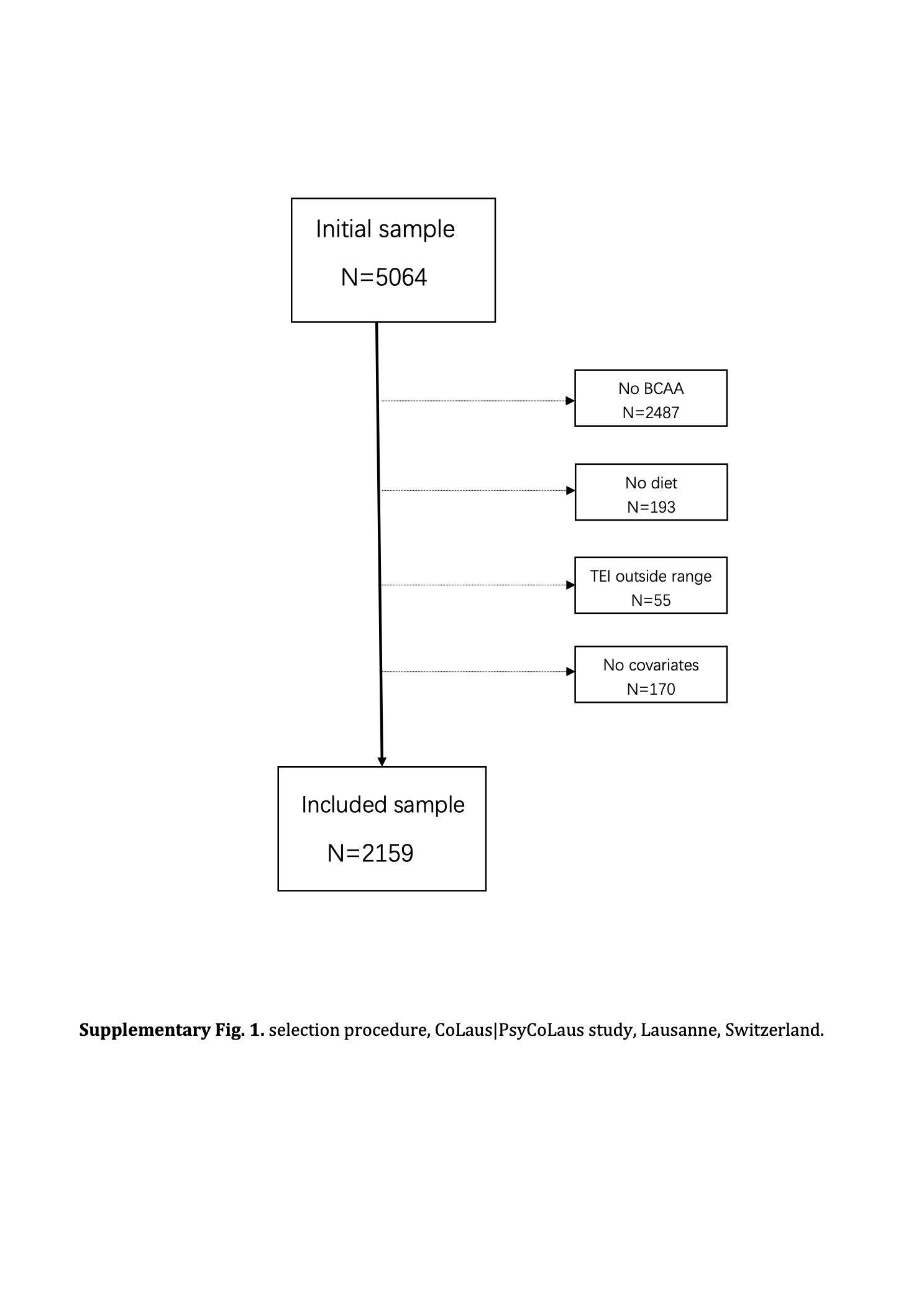
Eligibility and exclusion criteria
Participants with BCAA levels will be considered as eligible. Participants were excluded if they have no dietary markers, if they presented extreme total energy intake values (defined as < 500 or > 3500 kcal/day for women and < 800 or > 4000 kcal/day for men), if they missed any confounder variable or if they reported being on any type of diet (for slimming, antidiabetic, etc.).
Statistical analyses
Statistical analysis was conducted using Stata version 17.0 (Stata Corp, College Station, TX, USA). Summary statistics are reported as mean ± standard deviation for continuous variables and as number of participants (percentage) for categorical variables. Bivariate between-group comparisons were performed using t-test for continuous variables and chi-square for categorical variables. Normality of the distribution of BCAA was checked via Q-Q plots, and no deviation was found.
As dietary intake values presented with a skewed distribution, bivariate associations between dietary markers and the levels of circulatory BCAA were computed using Spearman correlations for the overall sample and stratified by gender. Multivariable regression analysis assessing the association between dietary markers and levels of circulatory BCAA were conducted using linear regression adjusting on age (continuous), smoking status (never, former, current), educational level (low, medium, high), marital status (yes, no), born in Switzerland (yes, no), presence of a diet (yes, no), BMI categories (normal, overweight) and sedentary status (yes, no). Results were presented as standardized beta coefficients, as their interpretation is similar to the correlation coefficients.
Bivariate analysis of the associations between dietary recommendations and levels of circulatory BCAA were assessed by comparing levels of circulatory BCAA between compliant and non-compliant participants using student’s t-test and the results were expressed as mean ± standard deviation, Multivariable analysis was conducted using analysis of variance, adjusting for the same variables as above, and results were expressed as multivariable-adjusted mean ± standard error. As this was an exploratory study, and similar to other studies(27, 28), we decided not to correct for multiple testing, and we defined statistical significance as a two-sided test with p < 0.05.
{kind=link}