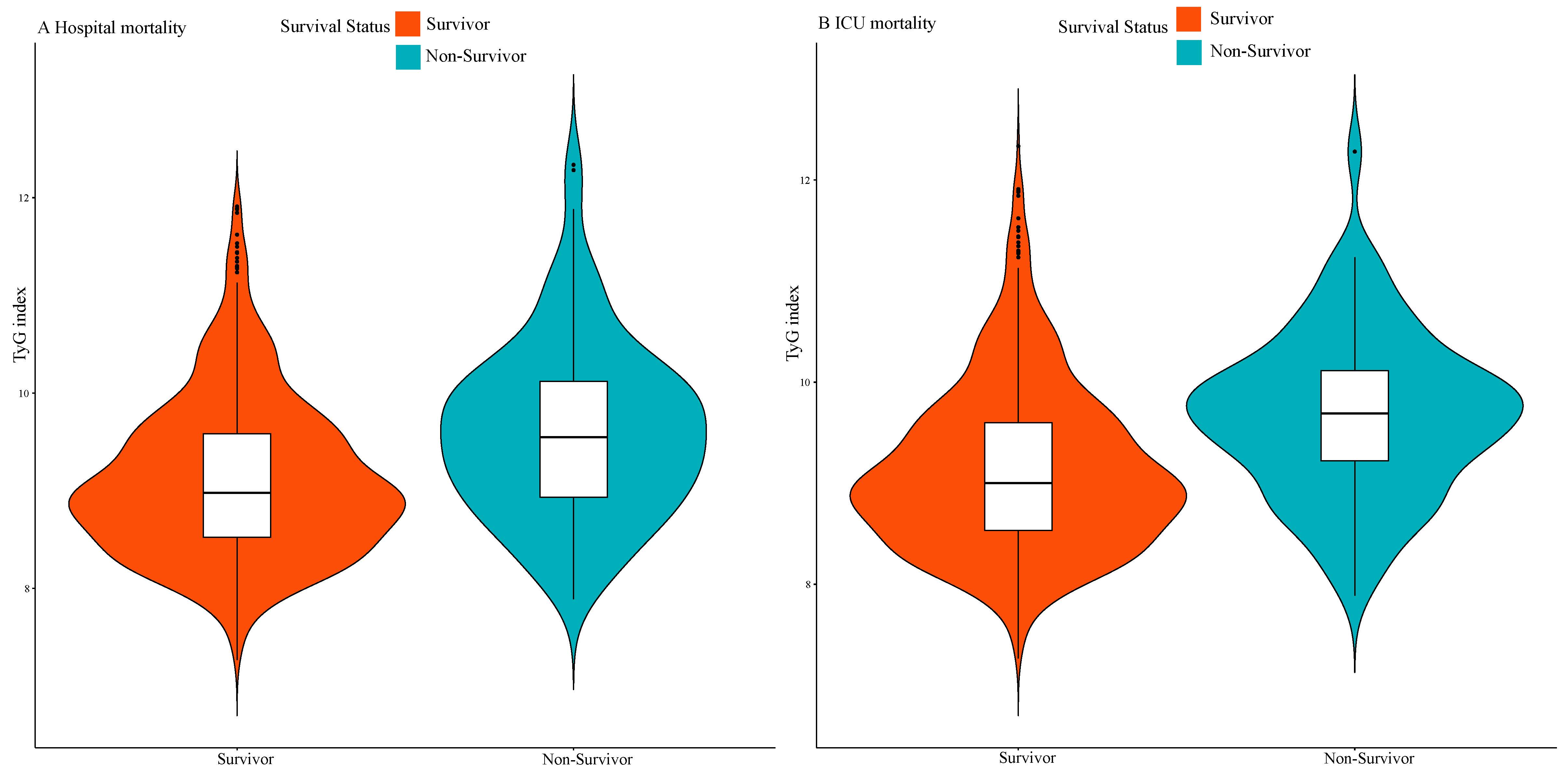
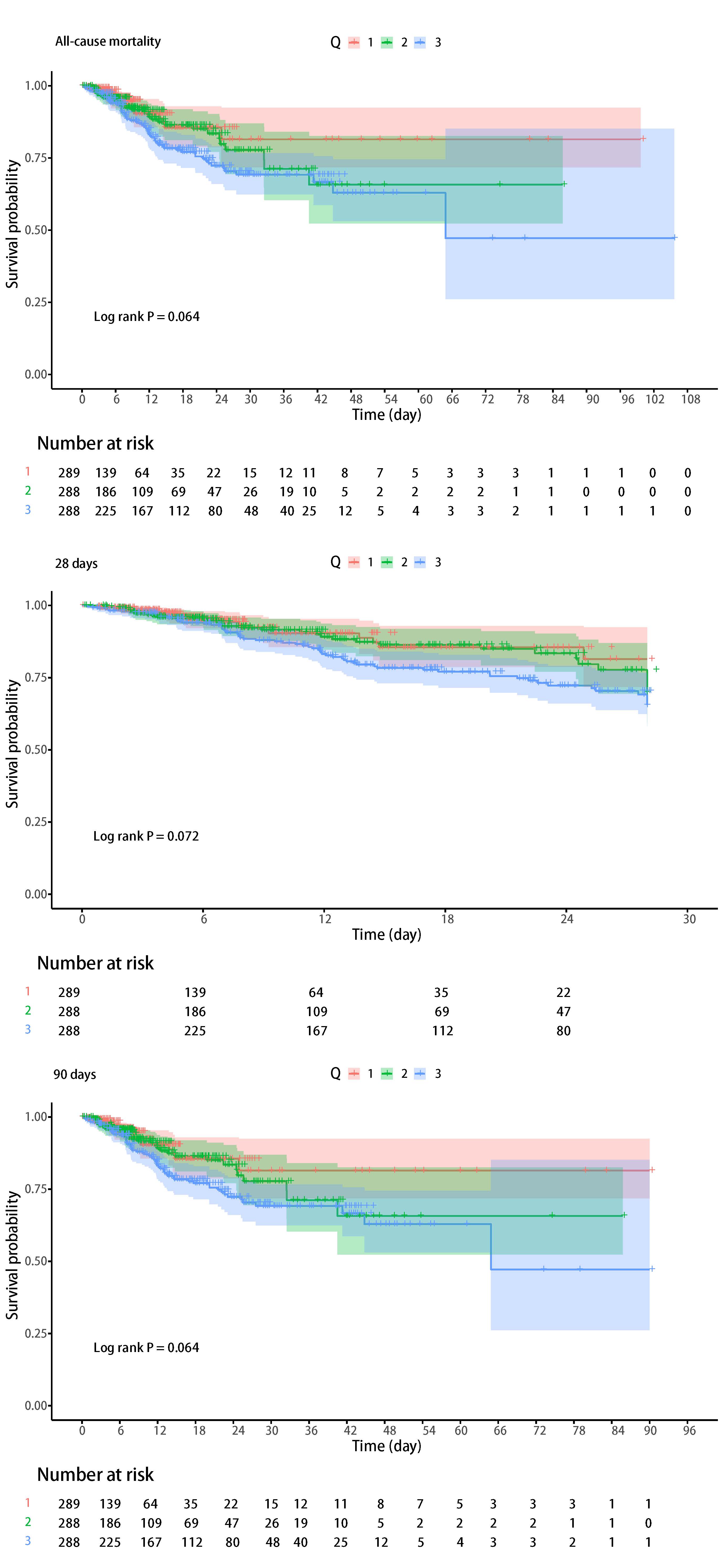
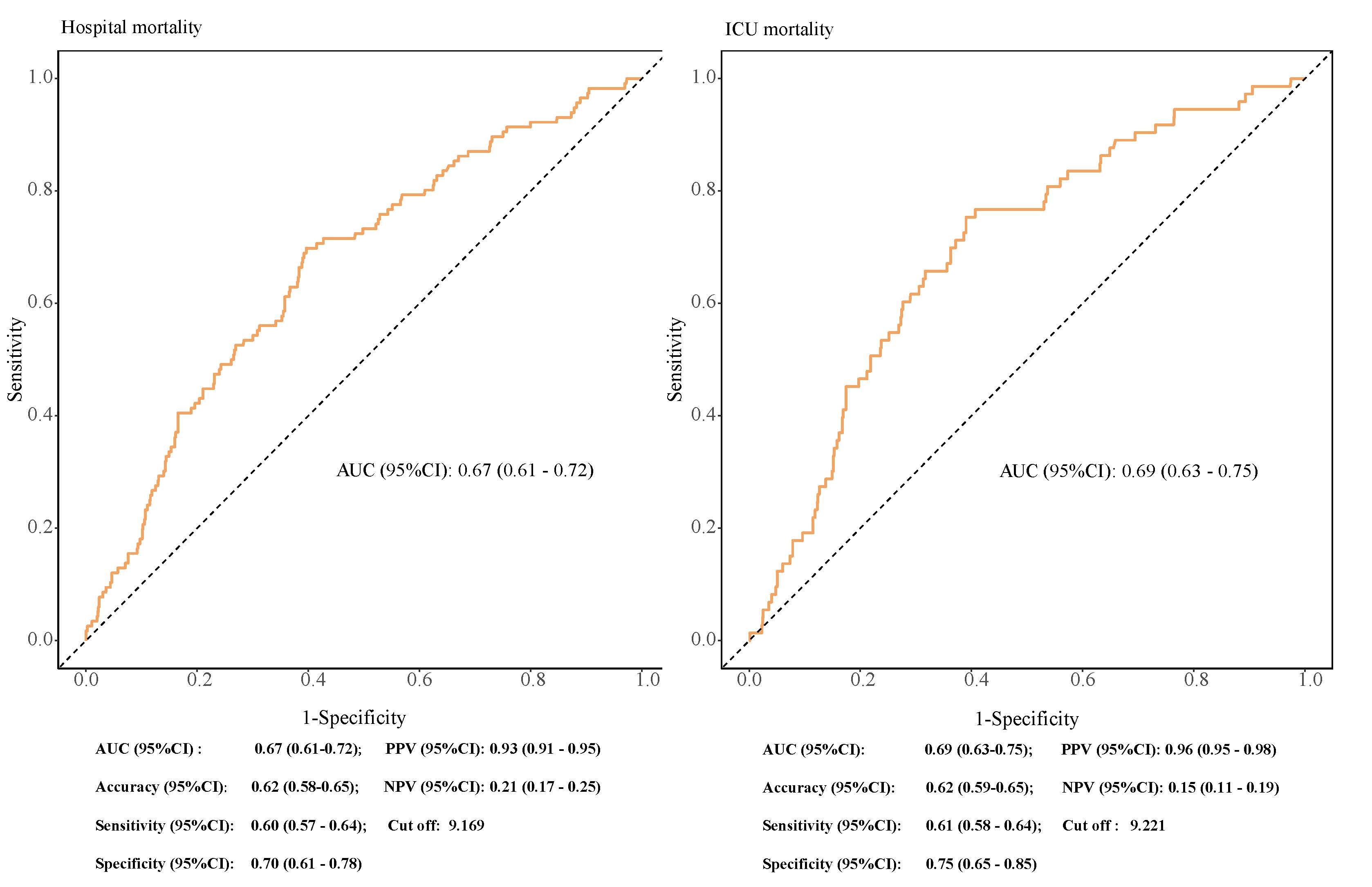
To the best of our knowledge, this study is the first to examine the relationship between the TyG index and clinical outcomes in TBI patients. Our findings suggest that a higher TyG index is associated with increased all-cause hospital and ICU mortality in critically ill TBI patients. Even after adjusting for confounding risk factors, the TyG index remained strongly associated with all-cause hospital and ICU mortality.
The TyG index, consisting of TG and FBG, has been suggested to be a potential indicator of metabolic disorders, atherosclerotic disease, cardiovascular disease, and hemorrhagic disease [13–16]. Numerous clinical studies have explored the associations between the TyG index and the incidence and mortality of cardiovascular diseases across various populations, including both public and specific patient groups. According to Yang et al., an elevated TyG index was associated with an increased risk of mortality in the hospital and ICU among patients who experienced cardiac arrest [17]. On the basis of the observations of Lee et al., the TyG index may help predict short-term functional outcomes in patients with acute ischemic stroke who have undergone reperfusion therapy [18]. Liu et al. revealed an association between the TyG index and mortality among surgical ICU patients [19]. In patients with sepsis, the TyG index could help in the early identification of insulin resistance, thereby improving risk evaluation and guiding further interventions [6]. Additionally, another study indicated that the TyG index might serve as a valuable predictor of future cardiovascular events in individuals with coronary artery disease [20]. These studies indicate that the TyG index holds promise for predicting the clinical outcomes of critically ill patients, patients with infection, and patients with cerebrovascular-related diseases.
The results of this study suggest an association between elevated TyG index levels and both the severity and clinical outcomes of TBI. TBI may lead to insulin resistance and impaired lipid metabolism, along with uncontrolled hyperglycemia and fluctuations in blood glucose during the acute phase [21–23]. The outcome of TBI is strongly correlated with the intensity of inflammatory responses, which are significantly related to insulin resistance. Our study revealed a positive association between the TyG index and the TBI.
The precise biological pathways that link the TyG index to TBI prognosis have not been fully elucidated. Research indicates that insulin resistance is associated with the TyG index. Insulin resistance may trigger the development of the dyslipidemia triad, which in turn facilitates endothelial dysfunction, the local release of chronic inflammatory mediators, endothelial injury, and eventually contributes to atherosclerosis development [24–26]. First, the TyG index may reflect the status of glucose metabolism, inflammation, and oxidative stress. In a state of insulin resistance, the production of nitric oxide (NO) stimulated by insulin is reduced. As a result, the inhibition of MAPK pathway activation due to hyperinsulinemia is impaired. Moveover, increased blood glucose levels combined with hyperinsulinemia further enhance the activation of the MAPK pathway, amplifying its downstream effects, such as heightened local inflammatory responses. Second, an increased TyG index may increase the level of free fatty acids, which may accompany insulin resistance. Chronic excessive calorie levels in the presence context of insulin resistance leads to increased visceral fat accumulation within the body [27]. Subsequently, adipocytes release chemokines, which induce monocytes to differentiate into macrophages that secrete large amounts of TNFα, reducing the storage of insulin-related substances. This leads to elevated circulating triglyceride levels and promotes an increase in free fatty acids [28]. All these pathophysiological changes can lead to poor clinical outcomes.
However, studies on the association between the TyG index and critically ill patients are rare. An elevated TyG index is significantly associated with an increased risk of mortality in critically ill patients with stroke and cardiovascular disease [6, 8, 29]. In our study, significant variations in APACHE scores were observed across patients grouped by their TyG index, suggesting a strong correlation between the TyG index and the severity of the disease. Furthermore, for TBI, we identified the TyG index as an important independent predictor of mortality in critically ill patients, contributing to clinical management aimed at reducing the risk of future adverse outcomes.
In addition, this study further analyzed the risk stratification of various subgroups. Our study revealed that the linear relationships between the TyG index and hospital mortality in TBI patients were consistent across older patients, female patients, those with higher BMIs, those without renal disease, those without atrial fibrillation, and those without stroke. This phenomenon could be explained by reverse causality: patients who are already diagnosed with these comorbidities are more likely to have received proper treatment or made healthy lifestyle changes. Interestingly, individuals with a higher TyG index tended to be younger, but the relationship between the TyG index and all-cause mortality was stronger in older patients, which is different from findings of previous studies. Consistent with common practice, clinicians tend to focus more on older TBI patients, as they are likely to have more comorbidities and face a higher risk of mortality. This study also revealed a clear linear association between the TyG index and hospital mortality, suggesting that the TyG index could serve as a practical tool for identifying critically ill TBI patients at high risk of mortality. Therefore, maintaining proper triglyceride and glucose levels, along with improved management of the TyG index, contributes to reducing the risk of future major adverse clinical events. In conclusion, our analysis suggests that the TyG index should not be viewed as the sole diagnostic measure but rather as a complementary tool alongside other clinical and laboratory parameters. This combined approach offers a more comprehensive evaluation of an individual's metabolic health and aids in the risk stratification of clinical outcomes, such as mortality in severe TBI, in clinical practice.
However, it is important to acknowledge the limitations of this study. First, our analysis was retrospective and conducted with observational data, and this study could not definitively establish causality. Although multivariate adjustment and subgroup analyses were used, residual confounding factors could still have influenced the clinical outcomes. Second, TBI itself could affect lipid metabolism and blood glucose fluctuations, and the TyG index may change significantly when a patient is in the hospital. Instead of relying solely on measurements that were performed at admission, future research should focus on monitoring this index dynamically throughout the treatment process. Finally, our study did not perform a hyperinsulinemia-euglycemic clamp test, so we cannot evaluate the association between the TyG index and the gold standard of insulin resistance assessment. Further research is needed to investigate the key mechanisms underlying insulin resistance in patients with TBI.
{kind=link}
{kind=link}
{kind=link}