Liver injury is associated with a poor prognosis in patients with COVID-19
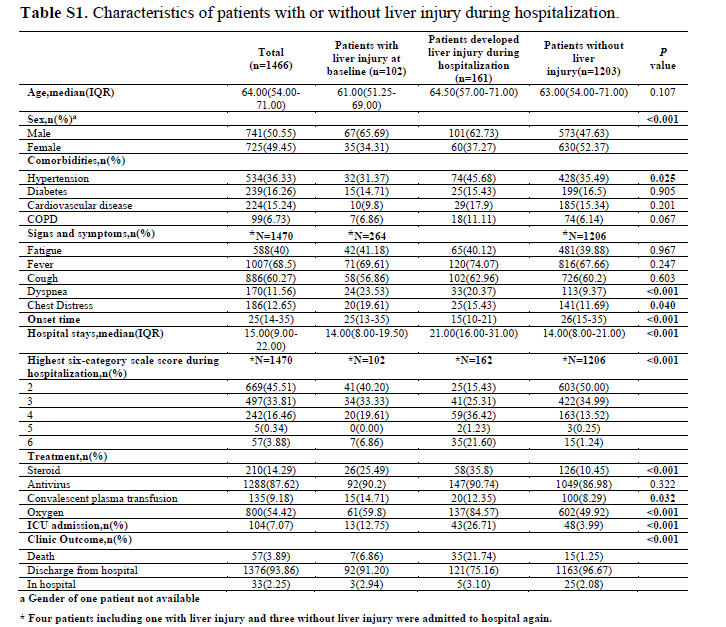
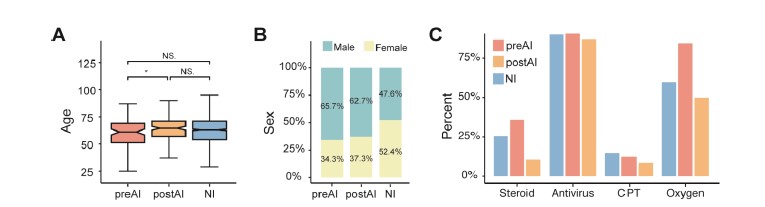
We identified 263 (17.9%) patients with liver injury (Table S1) to explore the impact of liver injury on severe or critical cases of COVID-19. Amongst these patients, 102 (38.78%) had presented with liver injury on admission (pre-admission injured group) and 161 (61.22%) patients developed liver injury during their hospitalization (post-admission injured group). As shown in Fig. 1A, hypertension was more commonly seen in the post-admission injured group (45.68%, p=0.025). The median time from symptom onset to admission was significantly shorter in the post-admission injured group than that in the pre-admission injured and non-injured groups (Fig. 1C, median:15 vs. 25 or 26 days, p<0.001), suggesting that disease progression was faster in the post-admission injured patients. The length of hospital stay was significantly longer in the post-admission injured group (Fig. 1C, median 21 days) than that in the other two groups (median 14 days for each). Furthermore, the six-category scale scores for the post-admission injured group were significantly enriched in the 3 to 6 range (Fig. 1D), indicating a higher risk. Conversely, over 50% of patients without liver injury remained at levels 2 and 3. The post-admission injured group also had significantly higher mortality rates than the pre-admission injured and non-injured groups during hospitalization (Fig. 1F, 21.74% vs. 6.86% or 1.25%, p<0.001), as well as increased intensive care unit (ICU) admission rates (Fig. 1E, 26.71% vs. 12.75% or 3.99%, p<0.001).
CLD is not significantly associated with a poor prognosis in patients with COVID-19
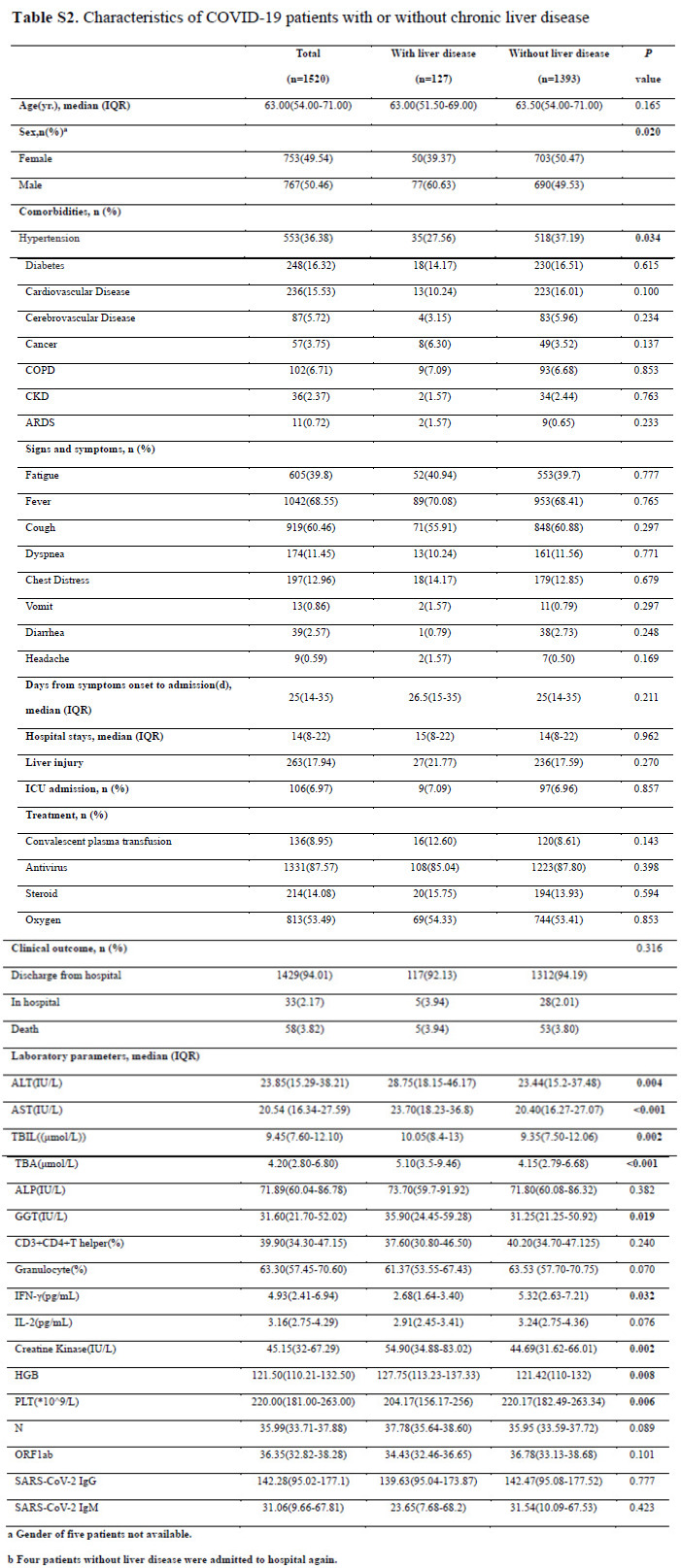
We compared the differences between severe or critical COVID-19 patients with and without CLD to evaluate the influence of SARS-CoV-2 on patients with pre-existing CLD. As shown in Table S2, 127 (8.35%) of the 1,520 patients with severe or critical cases of COVID-19 had CLD, including 64 patients with CHB, 20 with CHC, 37 with FLD, and 6 with liver cirrhosis but without documented etiological factors. Among all the comorbidities tested in this study, hypertension was the only one that showed a significant difference between the groups (27.56% with CLD vs. 37.19% without CLD, p=0.034).
Laboratory test results were also compared between the two groups. The median platelet count was significantly lower in the patients with CLD than that in those without CLD (206.00*10^9/L vs. 220.00*10^9/L, p=0.008). Interferon gamma was significantly decreased in patients with pre-existing CLD than that in those without pre-existing CLD (median: 2.68 vs.5.32 pg/mL, p=0.032). A similar trend was also observed for interleukin-2 and CD3+/CD4+ T-helper cell fractions, but these changes were not statistically significant.
No significant evidence of CLD being a risk factor for the severity or mortality of COVID-19 was found. This result may be due to the consistent and targeted delivery of liver protection treatments in patients with CLD. In addition, this result implies that liver injury occurring during the course of COVID-19 is associated with a poorer prognosis but pre-existing CLD is not.
Patients with FLD are at a higher risk of liver injury compared to patients with viral hepatitis
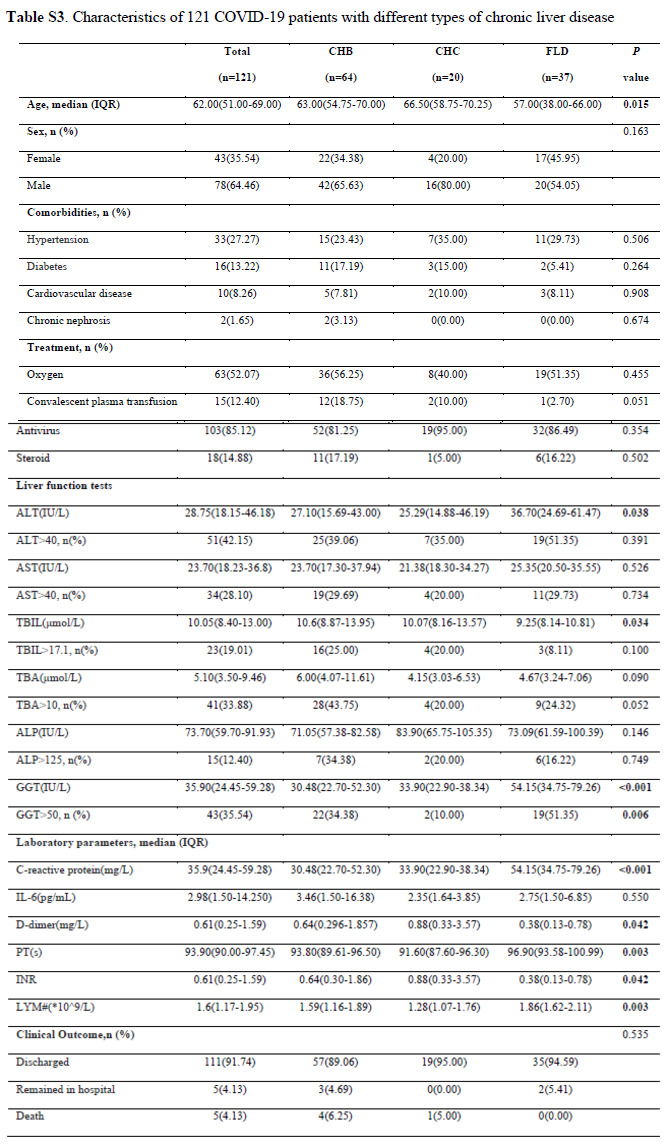
We conducted a comprehensive analysis of 121 patients with both COVID-19 and chronic liver comorbidities. Of these 121 patients, 64 (52.89%) had CHB, 20 (16.53%) had CHC, and 37 (30.58%) had FLD (Table S3). The clinical outcomes were not significantly different among the different types of CLD (p=0.535). However, all 5 recorded deaths occurred in patients with viral hepatitis. Patients with FLD had higher levels of ALT (median: 36.70 IU/L, p=0.038) and GGT (median: 54.15 IU/L, p<0.001) than those with CHB or CHC. Furthermore, over 50% of patients with FLD had abnormal levels of ALT (p=0.391) and GGT (p=0.006).
C-reactive protein (CRP) (median: 54.15 mg/L, p<0.001) and the absolute lymphocyte count (lymphocyte#; median: 1.86, p=0.003) were higher in the FLD patients. Prothrombin time was also significantly prolonged (median: 96.90 s, p=0.003) and the international normalized ratio was significantly lower in patients with FLD (median: 0.38, p=0.042), suggesting that coagulation disorders and dysfunction of the liver occurred concurrently in patients with pre-existing FLD. These results imply that patients with FLD suffer more severe liver damage.
Patients with both COVID-19 and cirrhosis are at a higher risk of disease progression
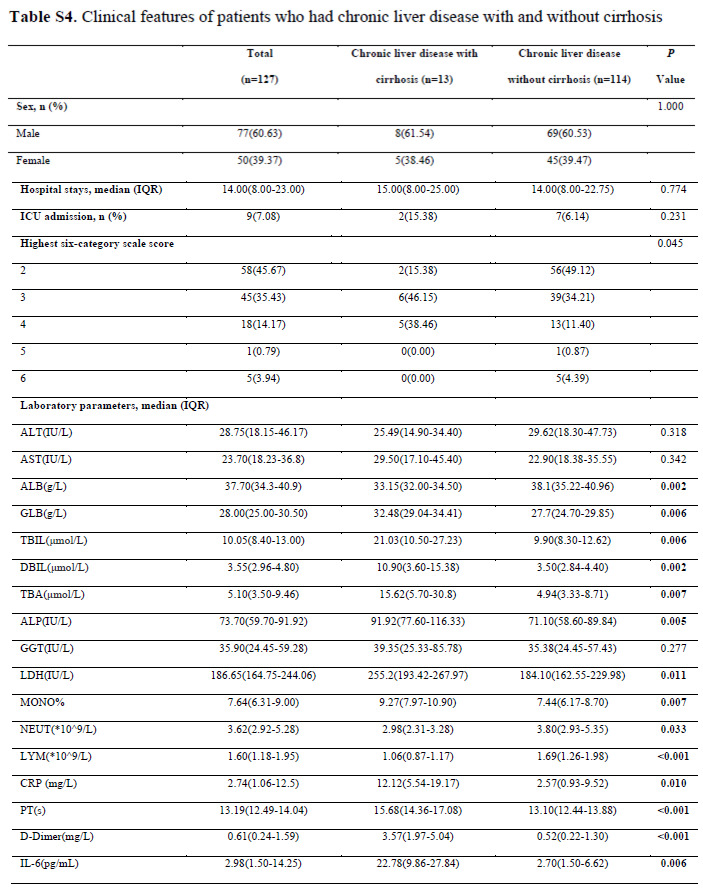
Cirrhosis is a complication of many liver diseases. Therefore, we analyzed the clinical characteristics and laboratory features of patients with CLD and with and without cirrhosis. As shown in Table S4, 13 (10.24%) patients had CLD with cirrhosis, of which 4 had CHB, 2 had CHC, 1 had MAFLD, and 6 had cryptogenic cirrhosis. No significant differences in terms of hospital stays (p=0.774) or ICU admission rates (p=0.231) were observed. However, the highest six-category scale scores for patients with both CLD and cirrhosis were significantly enriched at 3 and 4, while for those without cirrhosis were mainly at 2 and 3 (p=0.045). This result indicated that patients with both CLD and cirrhosis are at a higher risk of disease progression.
We confirmed by examining laboratory results that most liver enzymes were significantly higher in patients with cirrhosis, except ALT, AST, and GGT. Moreover, the levels of D-dimer and two well-known proinflammatory biomarkers (interleukin-6 and CRP) were found to be higher in patients with cirrhosis. All evidence mentioned above showed that patients with both COVID-19 and cirrhosis were at an elevated risk of disease progression compared with the patients who had CLD without cirrhosis.
Cirrhotic and fatty livers generate more TMPRSS2-expressing cells
We studied the liver scRNA-seq data in recent publications to investigate why patients with cirrhosis are more affected by SARS-CoV-2 (13, 14). Consistent with many recent reports, the level of the SARS-CoV-2 entry-receptor ACE2 was low in liver tissue. However, a small population of TROP2+ liver epithelial progenitors expressed ACE2 and the SARS-CoV-2 entry-associated protease TMPRSS2 (Fig. 2). Of the 11,106 cells detected in healthy livers, only 2 cells expressed ACE2 and 108 expressed TMPRSS2 (Fig. 2A). Of the 6,620 cells analyzed from cirrhotic livers, 7 cells expressed ACE2 and 143 expressed TMPRSS2 (Fig. 2B). This result represents a significant increase in the number of TMPRSS2-expressing cells in the cirrhotic livers (p<0.001, Fisher’s exact test). Of 7,244 cells analyzed from untreated HBV livers, only 1 cell expressed ACE2 and 35 expressed TMPRSS2 (Fig. 2C). The TMPRSS2-expressing cells were significantly fewer in HBV liver than those in both healthy and cirrhotic livers (p<0.001, Fisher’s exact test) (Fig. 2D).
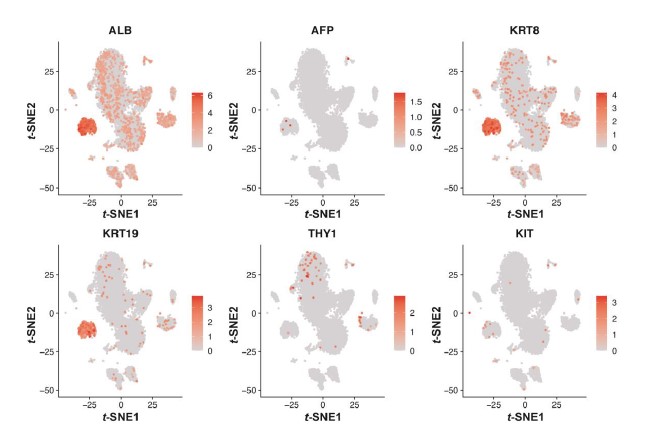
We estimated the abundance of TMPRSS2+ progenitor cells for other liver bulk expression profiles with CIBERSORTx using the signatures built from the same healthy liver scRNA-seq dataset. To obtain a better reference signature, we limited TMPRSS2+ progenitor cells to a subset of the cell population in “cluster 4” marked by markers ALB, KRT8, and KRT19 (Fig. S2). Compared to HBV and HCV infected livers, MAFLD livers had much higher TMPRSS2+ progenitor cells (Fig. 2E) indicating that MAFLD livers might be more susceptible to the SARS-CoV-2 virus. Similarly, the cirrhotic livers also had higher TMPRSS2+ progenitor cells than healthy livers, which is comparable to the scRNA-seq results.
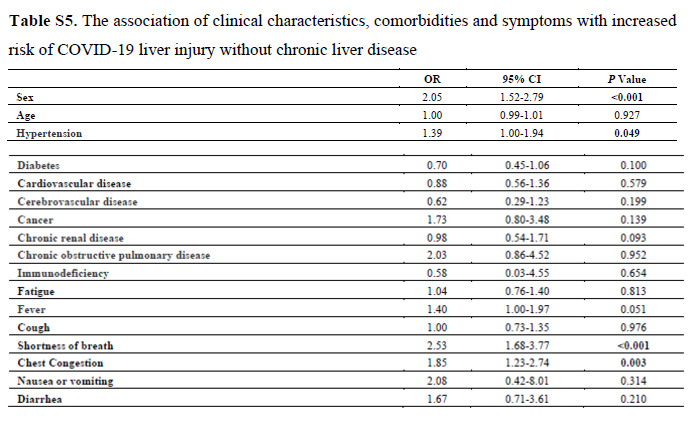
Hypertension may increase the risk of liver injury for patients without pre-existing CLD
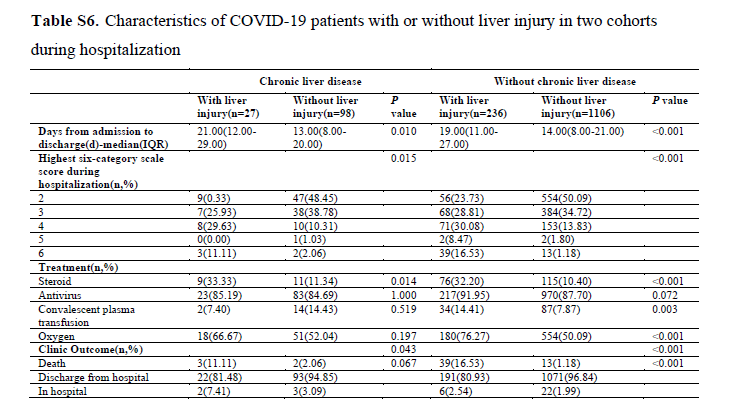
A logistical regression model was used to identify the clinical characteristics, comorbidities, and symptoms that could increase the risk of liver injury among patients without pre-existing CLD. As shown in Fig. 3, male sex was highly associated with the risk of liver injury suggesting that male patients are more likely to develop liver injury (see Table S5 for details). Furthermore, the association of hypertension and liver injury was significant for patients without pre-existing CLD but not for patients with pre-existing CLD (Table S6).
Risk scoring model for assessing liver injury and clinical outcomes for COVID-19 patients
We built a risk scoring system based on 22 routine laboratory tests performed within 3 days after admission, such as liver function and routine blood tests. This system was used to evaluate the risk of liver injury in patients with COVID-19 as early as possible and provide guidance for the management of these patients. The univariate logistic regression model was applied to select potential laboratory parameters, and only those with an OR >1 and p-value <0.001 were retained for final modeling. We selected 3 indicators at admission, including ALT (OR 1.07, 95% CI 1.02-1.12), CRP (OR 1.02, 95% CI 1.01-1.04), and LDH (OR 1.29, 95% CI 1.20-1.39). Fig. 4A shows the distribution of tested values for selected indicators. To determine the robustness of this model, a 5-fold cross-validation method was employed. The average AUC of 5-fold cross-validation was 85% (Fig. 4C). Similarly, we selected 6 indicators (Fig. 4B) to predict whether patients would proceed to six-category scale scores of 5 or 6. The average AUC reached 92% (Fig. 4D). An R-package provides all operations required for the clinical outcome prediction of new patients (https://github.com/liangyuan-njmu/PredictModel).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}