The UCTP was conducted between 1 to 14 September 2020 in 148 test centres across all 18 districts of Hong Kong (Figure 1A). In total, 1,783,232 samples were tested from 1,765,549 individuals (24% of the total population), including a very small number of repeated samples (1%) from the same individuals (Table S4). Age and sex were available for 99.8% of the samples, of which 70.0% were aged between 20 to 64 years old (Table 1).
The district- and age- specific participation proportions were broadly consistent with the corresponding preceding incidence of confirmed COVID-19 cases (Figure 1). The districts of Wan Chai and Central and Western had the highest participation proportion (39% and 32%, respectively) but lower preceding incidence compared to the other districts (Figure 1B). Although adults aged 20 to 29 had a high preceding incidence, their participation proportions (8.9% and 11.0% respectively) were the lowest among all eligible age groups (Figure 1C). Consistently, we found relatively lower intention to participate (26.2%, 95% CI: 20.1%, 33.0%) and a higher proportion of concerns about participation in the UCTP in adults 18 to 39 years of age compared to other age groups in the telephone survey (Figure 2).
The UCTP identified a total of 40 individuals with a positive RT-PCR result. Among them, 32 were newly identified COVID-19 cases, and 8 were recovered individuals from previously confirmed COVID-19 who were determined by public health officers to have long-term virus shedding rather than re-infections. All these 8 recovered cases with long-term shedding, comprising1.3% (95% CI: 0.6%, 2.6%) of 611 recovered were tested in the UCTP, were not thought to be infectious at the time of testing as they were discharged from hospital within the preceding month following complete symptom resolution and had detectable IgG antibodies. As such, these 8 cases were not included in further analyses.
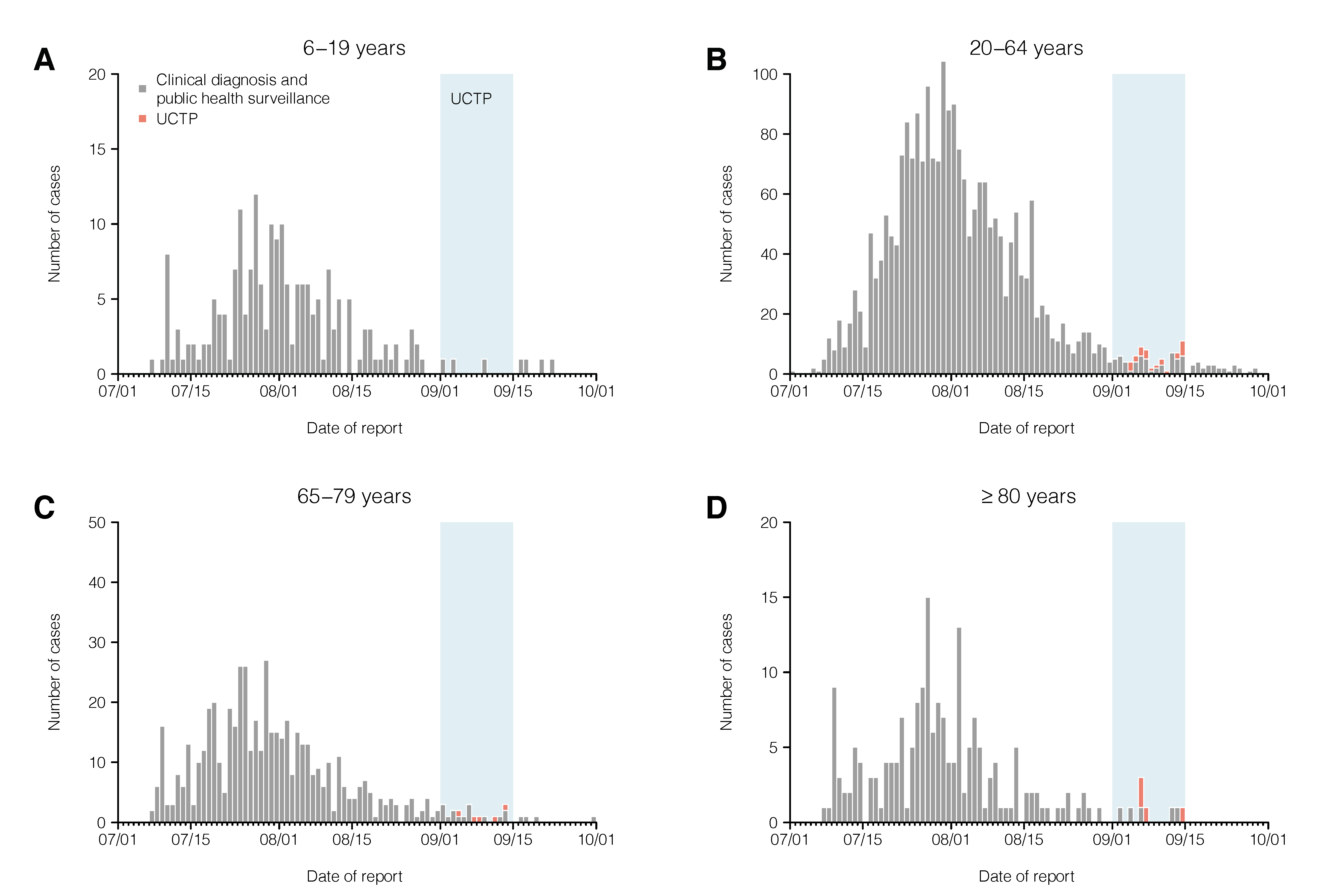
The 32 newly-identified cases represented 29% (95% CI: 21%, 38%) of the 111 local cases that were identified during the two-week UCTP program (Figure 3A). The proportion of test positives of the UCTP was 1.8 (95% CI: 1.2, 2.5) per 100,000 samples tested, with the highest proportions among people aged over 80 years of age (6.6, 95% CI: 1.8, 16.8 per 100,000; Table 1). Ct values were similar between cases detected in the UCTP and those from the clinical diagnosis and public health surveillance (geometric mean 27.2 vs. 25.0, Mann-Whitney U test, p = 0.26) (Figure 4A).
Among the 32 newly identified cases, 41% (n = 13) had no symptoms at the time of testing, which was similar to that (29%, 23 out of 79; chi-squared test, p=0.34) among cases detected from existing surveillance during the UCTP period (Figure 3). Of note, 4 cases developed symptoms on or after the day of the test. The median length of hospital stay was similar between cases detected by the UCTP and those detected from existing surveillance in September (9.5 vs. 11 days, Wald test under a Cox regression model, p = 0.77) after adjusting for age (Figure 4B).
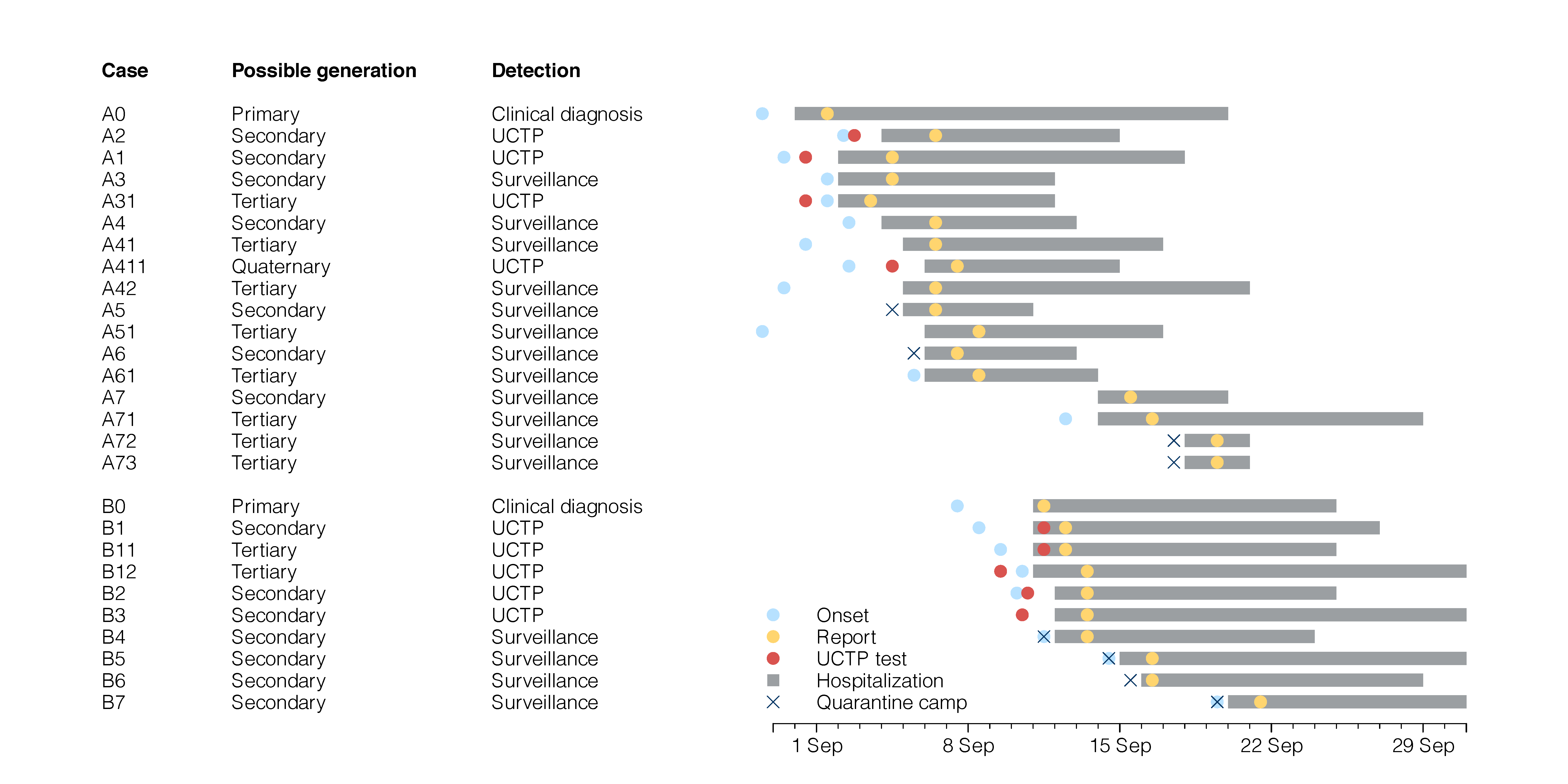
About 62% (n = 20) of the newly identified cases from the UCTP had no epidemiological link with any other confirmed COVID-19 cases as their potential infectors, which was higher than those (27%, 21 out of 79; chi-squared test, p<0.001) detected from the clinical diagnosis and public health surveillance during the same period. Among these 20 possible primary cases, 70% (n = 14) did not appear to transmit to any individual. Two of them (out of 20, 10%) transmitted to three of their household members who were also detected in the UCTP, and four (20%) transmitted to household members who were later detected through contact tracing (Figure 3B). These six transmission chains consisted of 33% (n = 18) of the newly identified transmission chains during the UCTP period. Nine of the newly confirmed cases were found to have epidemiological links to two known clusters identified by the existing surveillance, and five were contacts of the possible primary cases of the clusters, suggesting at least 35.7% (95% CI: 12.8%, 64.9%) of the possible secondary cases in the two clusters might have been missed by contact tracing (Figure 3B).
By comparing cases identified through the UCTP and the existing clinical diagnosis and public health surveillance, we were able to estimate the proportion of all infections that were being detected by the existing surveillance. In our Bayesian modelling analysis, we estimated that the incidence of infections during the third wave was 1.3 (95% credible interval (CrI): 0.6, 2.8) per 1,000 for individuals 6 to 19 years old, 1.5 (95% CrI: 1.2, 2.0) per 1,000 for aged 20 to 64, 1.9 (95% CrI: 1.4, 2.5) per 1,000 for 65 to 79 and 2.5 (95% CrI: 2.0, 3.2) per 1,000 for those at 80 years of old or above (Figure 5A). We estimated a total of 12,000 (95% CrI: 9,800, 15,000) infections occurred in people aged above 6 years in the third wave in Hong Kong, suggesting an overall 27% (95% CrI: 22%, 34%) of all infections were detected by existing surveillance during that period. The highest proportion of detection (56%, 95% CrI: 50%, 61%) was in persons aged 20 to 64 years old (Figure 5B), who were also more likely to be detected as “possible primary” cases compared to other age groups (Table S5).

{kind=link}
{kind=link}
{kind=link}