In an effort to predict OSA risk among Chinese adults, we herein developed a predictive model based upon eight objectives, easily measured variables associated with OSA incidence (Gender, BMI, HTN, DM, Cr, BUN, SUA and TG). In total, 120 patients were evaluated to develop this model, with 18 variables including demographic data, laboratory findings, ultrasound results, and comorbidities being assessed via a LASSO approach to screen for significant risk factors linked to OSA incidence. The resultant predictive model exhibited good discrimination upon intra-cohort validation, with high C-index and AUC values suggesting that this model can be widely applied to screen for OSA risk.
Sex, age, obesity, snoring, pharyngeal abnormalities, and cephalometric features have all been identified as OSA-related risk factors in the general population [12, 13]. OSA rates are higher among males in regional surveillance studies [14], consistent with the identificaiton of male sex as an independent predictor of OSA risk [15–17]. This may be linked to the fact that males are more likely to exhibit central weight gain than are females, leading to more upper airway fat storage [18]. Hormones may also influence OSA pathogenesis, as evidenced by the fact that it is more common among post-menopausal women relative to pre-menopausal women [19, 20]. In line with our results, OSA is known to be among the strongest risk factors for OSA, with over half of all OSA diagnoses being linked to an individual being overweight [21]. OSA rates have been found to be positively correlated with BMI [22], and one group reported that a 10% increase in weight was associated with a 32% increase in AHI scores, thus contributing to more severe OSA [23]. Obesity is thought to contribute to OSA incidence both through reductions in lung volume and increases in fat deposition within the neck and other soft tissue regions [24]. Other factors that can influence OSA development include changes in the neural compensatory mechanisms responsible for maintaining airway patency, respiratory control system instability, and decreased functional residual capacity [25]. The implementation of more effective weight loss strategies is thus critical to reduce the incidence of OSA in the general population.
With respect to comorbidities, HTN has been linked to OSA risk in several reports [15, 26–29]. Both SBP and DBP are reportedly positively correlated with AHI values and negatively correlated with nadir nocturnal oxygen saturation [30]. DM is also commonly associated with OSA, with the Wisconsin Sleep Cohort Study have demonstrated an independent association between DM and OSA [31]. The mechanistic basis for this relationship may be that DM can impact OSA-related periodic breathing [32], although furth research is necessary to fully understand how interactions between HTN, DM, and other conditions can affect OSA incidence.
Bouloukaki et al. previously reported that blood biomarkers may be of value when assessing individual risk of OSA [33], and OSA biomarker screening in high-risk populations has been linked to significant improvements in sleep specialist referrals and associated patient outcomes [34]. As such, our predictive model included Cr, BUN, SUA, and TG as blood biomarkers. SUA in particular has been previously identified as an independent predictor of OSA incidence, with each 1 mg/dL rise in SUA concentrations being associated with a 16% increase in OSA risk. Consistently, SUA was independently associated with OSA severity in a large study of OSA patients without known comorbidities [33], and there is evidence to suggest that hyperuricemia may promote oxidative stress and endothelial dysfunction, thereby favoring OSA development [35].
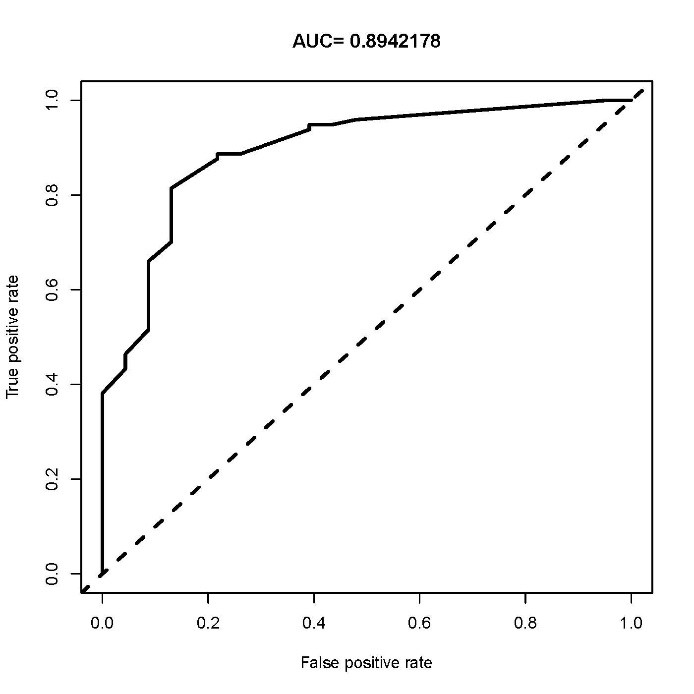
Multiple models capable of predicting OSA risk have been reported to date. For example, James et al. analyzed 370 participants and developed a predictive model with AUC values ranging from 0.669–0.757 based upon AHI [36]. Seon Tae Kim et al. employed a logistic regression analysis approach to establish two predictive models with AUC values of 0.782 and 0.809 [37], while Do-Yang Park et al. used a large-scale study to develop two models with and without physical examination data yielding respective AUC values of 0.835 and 0.839, respectively, although they did not analyze blood biomarkers in their model [38]. Relative to some of these previously proposed predictive models, ours had a higher AUC value, and our internal validation results exhibited excellent consistency among patient cohorts.
The nomogram developed herein (Fig. 2) is a simple tool that relies upon complex statistical models to enable the efficient quantification of personal OSA risk in a clinical setting. Vertical lines are drawn from the appropriate point on each clinical variable scale to the corresponding ‘points’ scale, after which all points values were summed, and another vertical line was drawn from the ‘total points’ scale to the ‘Risk of OSA’ scale in order to establish patient risk. For example, for a male patient (42 points) with obesity (52 points) and an SUA ≥ 416 umol/L (55 points), this nomogram predicted an OSA risk value of 0.58. Overall, this nomogram can aid in the identification of individuals at a high risk of OSA, supporting early intervention. Importantly, all of the variables that compose this predictive model are both objective and easily analyzed such that this model can be readily utilized to screen for OSA risk in the general population.
However, there are still several limitations in our study. This is a cross-sectional study with a small sample size and single center, which could not represent all the Chinese population. In addition, although the authenticity of our model was affirmed by internal validation, external validation could not be conducted. Therefore, this prediction model needs to be further verified by a longitudinal, multicenter and large sample study.
{kind=link}
{kind=link}
{kind=link}