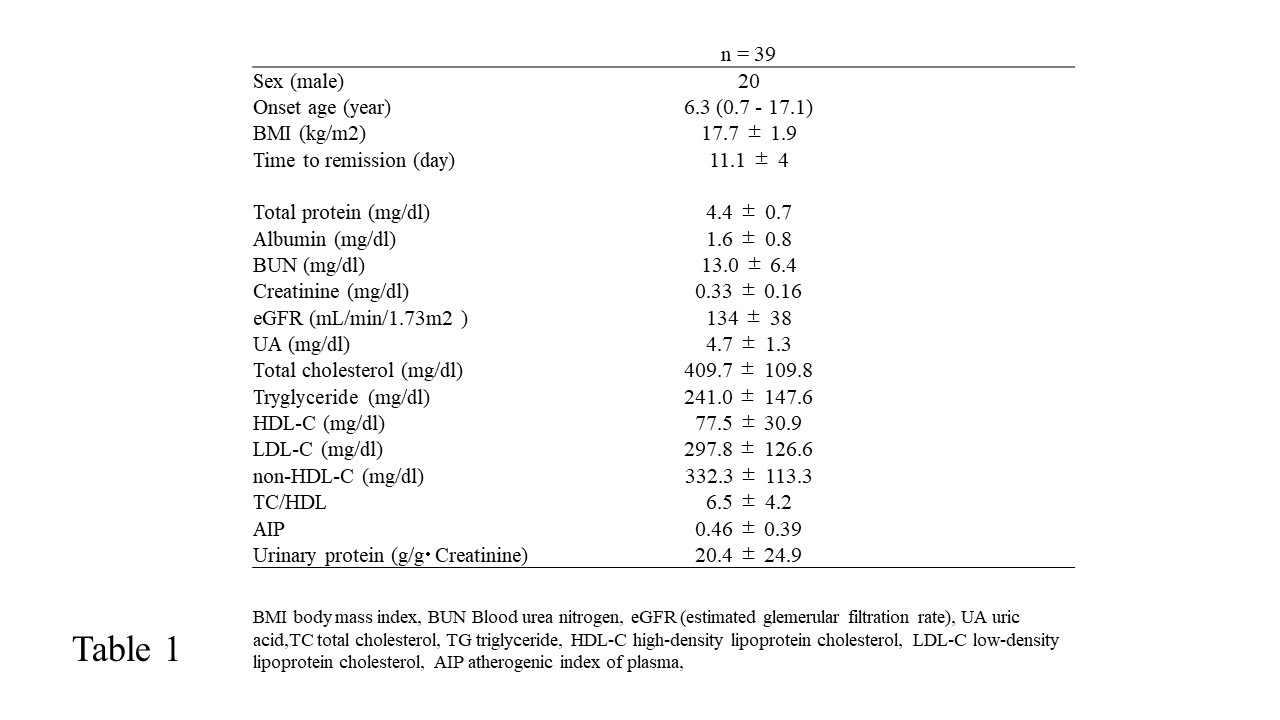
It is well known that TC, TG, and LDL-C levels are markedly increased during the nephrotic state. Especially in the initial onset, dyslipidemia appears frequently compared to that during the relapse phase. The magnitude of dyslipidemia in NS is considered to be directly associated with the severity of proteinuria [18]. In our study, significant dyslipidemia with not only high levels of TC, TG and LDL-C, but also non-HDL levels were noted. Non-HDL-C exhibits several benefits beyond LDL-C and can be used for lipid management when a patient’s samples show a TG level of > 400 mg/dL or non-fasting state [19]. As unifying the fasting samples at the onset is difficult, evaluating non-HDL-C level is considered to be useful, especially in children. Several studies reported high non-HDL-C levels in patients with metabolic syndrome. In our study, the non-HDL-C level of patients with NS was significantly higher than previously reported data [20, 21]. Furthermore, we focused on the LDL particle size to evaluate non-HDL-C level. TG is a powerful inverse determinant of LDL particle size [9, 17]. In other words, the higher the TG value, the smaller the particle size of LDL, which is recognized as sdLDL. Using the “alternative LDL window,” understanding the condition of dyslipidemia at a glance in the acute phase of NS is easy. When patients belong to the area of hyper-TG/-non-HDL, it implies that among those patients with sdLDL, 82% with hyper-TG/-non-HDL levels could be exposed to the risk of endothelial cell damage.
Endothelial cell damage contributes to the enhancement of vascular permeability, and it is considered to be one of the important factors in the development of NS. Sharma et al. reported that patients with SRNS exhibited high levels of endothelial dysfunction markers [22]. sdLDL is a lipoprotein that strongly induces arteriosclerosis and is closely associated with cardiovascular events. Using these criteria, the majority of our patients were found exhibit a considerable risk of developing premature vascular disease. Hyperlipidemia is also involved in the pathogenesis of various acute complications in NS [23, 24]. Interestingly, Ambrosch et al. provided novel clues on the atherogenic mechanisms of sdLDL, which sensitize vascular cells to inflammatory signals more effectively than normal-sized LDL particles [25]. The oxidative modification of LDL plays a vital role in the pathogenesis of several vascular diseases [26, 27]. In addition, endothelial dysfunction and inflammation occur in even an asymptomatic proteinuria state [28]. AIP is used to predict the angiographic complexity of peripheral artery disease, and it has been confirmed to be significantly correlated with other important atherosclerosis indexes such as LDL-C particle size and sdLDL-C [16, 29]. It was classified into 3 risk levels for CVD according to the following values: −0.3 to 0.1 for low risk, 0.1–0.24 for medium risk, and > 0.24 for high risk [30]. In our study, 69% of the patients exhibited high levels of AIP, which implies they may exhibit a high-risk condition during the acute phase, although it may be a short period. Clinically, no obvious complications were observed in both acute and remission phases in our study. This is not surprising as children basically do not present with an underlying illness and may demonstrate fewer complications than adults. In our study, we found that AIP positively and significantly correlated with lipid profiles such as TG, LDL-C, and TC/HDL negatively correlated with TP and Alb. The latter findings generally normalize, and hyperlipidemia also tends to disappear with the resolution of proteinuria. However, some studies reported persisting lipid anomalies during remission [31, 32]. In one study of 30 patients with childhood-onset steroid-sensitive NS (SSNS), dysregulation of lipids, including increased TC levels, and LDL-C were persistent during the follow-up at 4–15 years after the completion of steroid therapy [33]. The hyperlipidemic profiles remained despite the remission, especially in frequently relapsing NS cases [31]. Furthermore, subclinical cardiovascular disease and its association with risk factors are detected in children with SRNS [14]. In addition, lowering cholesterol levels using HMG-CoA reductase inhibitors during childhood may reduce the risk for atherosclerotic changes [34]. Hence, lipid-lowering agents may be of benefit in certain patients with NS such as those with SRNS.
Currently, the number of young patients improving from pediatric to adult renal care progressively increased due to improved management worldwide. It appears possible that even SSNS, which was previously believed to be entirely benign, may engender an increased risk for hypertension, atherosclerosis, and CKD in adulthood [35]. In our study, no significant correlation existed between the data of lipid profiles and eGFR. However, the CKD in Children Study reported that the presence of dyslipidemia was associated with the reduction of eGFR in patients with nonglomerular disease [36].
The limitations of this study include the small number of patients. Further studies are required to examine the changes in the levels of lipid profiles in individuals at the remission phase, which could help predict the severity and prognosis. In addition to increasing the number of patients, considering the measurement of aortic pulse wave velocity, carotid intima media thickness, and left ventricular mass is necessary to evaluate the risk factors of cardiovascular disease.
{kind=link}