Due to the increasing popularity of vaping products, the need to research possible health consequences related to using e-cigarettes has emerged. Many clinical cases suggest that vaping can have a detrimental impact on the respiratory system [1][2][3][4]. Electronic cigarettes are noncombustible tobacco products known also as ENDS (electronic nicotine delivery systems). Electronic cigarettes consist of a battery, a coil (the heating element) and a liquid solution (refill fluid) [5]. Electronic cigarette’s liquids (ECLs) within the device must be heated to the high temperature to form vapor, which is inhaled by an e-cigarette user. Mechanisms of cell impairment are still under research, but many of them are already known. Common symptoms of EVALI, which is e-cigarette or vaping product use-associated lung injury, are cough, dyspnoea, chest pain, fever, and gastrointestinal symptoms such as nausea, diarrhea, vomiting[2][6]. Histopathological examination revealed patterns of acute lung injury, including acute eosinophilic pneumonia, acute fibrinous pneumonia, diffuse alveolar damage, organizing pneumonia, usually bronchiolocentric and accompanied by bronchiolitis, acute respiratory distress syndrome (ARDS), diffuse alveolar hemorrhage, hypersensivity pneumonitis, peribronchiolar granulomatous pneumonitis and the rare giant-cell interstitial pneumonitis (Fig. 1) [2][7].
Depending on the chemical agent and the frequency and quantity of inhalation exposure symptoms may range from respiratory tract irritation (cough) to acute airway injury and damage to the parenchyma with pneumonitis, alveolar edema, respiratory failure and death [7]. National cross-sectional online survey dedicated for U.S. young adults showed correlation between vaping and SARS-CoV-2 infection. Ever-dual-users of e-cigarettes were 7 times more likely to be diagnosted with COVID-19 [9]. Ever-users of e-cigarettes were 5 times and past 30 days dual-users were 6.8 times more likely to be diagnosted with COVID-19 [9]. Nevertheless, another study showed no association between smoking and increased risk of SARS-CoV-2 infection[10].
The significant change in pulmonary function tests in e-cigarettes users was observed. Forced expiratory volume in 1 second (FEV1) and forced expiratory volume in 1 second to forced vital capacity ratio (FEV1/FVC) were both significantly reduced [11]. Forced expiratory flow (FEF) 25%, FEF 50%, FEF 75%, FEF 25%-75% and FEF 75%-85% were also significantly decreased [11]. Morphological and functional abnormalities related to vaping vary depending on factors which are not yet known.
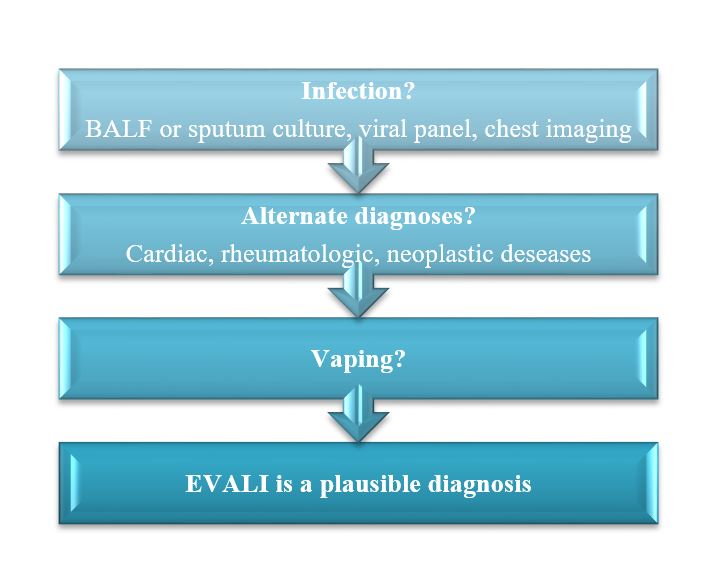
EVALI is a diagnosis of exclusion. Initially the respiratory (bacterial, viral or fungal) infection and other alternative diagnoses must be excluded (scheme 1) [6][12][13]. The viral panel includes influenza A and B virus, parainfluenza virus 1, 2 and 3, respiratory syncytial virus, adenovirus, rhinovirus, enterovirus [14]. SARS-CoV-2 infection must be also excluded.
Risk Factors Of E-cigarettes Use
Most patiens diagnosed with EVALI admitted using THC-containing products. It implies that (-)-trans-D9-tetrahydrocannabinol (THC) may be the main factor in pathogenesis of EVALI [15][16]. A small percentage of patients suffering from a vaping-associated lung injury denied using THC-containing products, which implies that there are more detrimental agents [17].
Nicotine
Nicotine (3-(1-methyl-pyrrolidinyl)-pyridine) concentration in ECLs may range from 0 to 20 mg/ml (the highest permissible concentration in the European Union and United Kingdom) [18]. For comparison, the average nicotine content in a classical tobacco smoke is 13,5 mg [19]. Nevertheless, the nicotine delivery profile is disparate. The pH of the refill fluid and the effectiveness of nicotine aerolization must be considered [5]. The pH of refill fluids can vary. Nicotine occurs in protonated form at acidic pH and free-base in alkaline fluids [5][20]. The nonionized form (free-based) is lipophilic and more bioavailable [21][20]. Also flavorings may affect the nicotine delivery profile. Menthol inhibits nicotine metabolism [22][23]. Menthol is a flavoring frequently used in tobacco products. Slowed nicotine metabolism increases nicotine exposure and toxicity. Menthol concentration in ECLs is higher than in combustible tobacco products [24]. Menthol (0,2 mg/ml) decreases human bronchial epithelial cells (BEAS-2B) proliferation [25].
Vitamin E Acetate (Vea)
Vitamin E acetate was considered to be the potential causative agent for EVALI [7][8]. VEA was found in bronchoalveolar lavage (BAL) fluid of many patiens who developed EVALI [28][29][30]. VEA is a lipophilic diluent used mostly in THC-containing products. Although it is said to be non-toxic as a food additive (oral intake), potential inhalation toxicity is unknown. Animal studies indicate a correlation between inhaling VEA and pulmonary injury. The level of albumin and the total leukocytes number were significantly increased in bronchoalveolar lavage fluid of mice exposed to VEA aerosol [27]. BEAS-2B cells exposed to VEA aerosol intensified reactive oxygen species (ROS) production [31]. Elevated concentration of inflammatory mediators (IL-6 and eotaxin) was detected in mice BALF after exposure to VEA [31]. Nevertheless, the Centers for Desease Control and Prevention (CDC) recommends not to add VEA to any e-cigarette or vaping product.
Temperature
Another risk factor is high temperature needed for the vaporization process. Heating coils within e-cigarettes enable wide temperature range. Vitamin E acetate upon pyrolysis forms highly toxic keten [32][33]. Keten is a gaseous substance which is proved to be a very high pulmonary toxicant, deadly at higher dose. At lower concentration causes respiratory irritation in animal studies. After heating ECL to the temperature that enables to form aerosol, toxic hydrocarbons and reactive aldehydes are made. Formaldehyde, acrolein and cinnamaldehyde are respiratory irritants. Vapor from cherry-flavored liquids contains more benzaldehyde than a tobacco smoke [34].
Trace Metals Contamination
Heating coils and tanks of e-cigarettes are made of metals. Under the high temperature within device those metals are released to liquids or e-cigarettes vapor. The content of lead, cadmium, chromium, cobalt, arsenic, antimony, manganese, tin, nickel, zinc, copper, aluminium, iron, tungsten and barium in ECLs or vapor has been already proved [35]. Chromium and nickel are considered to be the most significant metal contaminants. High concentration of nickel was found in ECLs, even higher than in classical tobacco smoke. Nickel is a human respiratory carcinogen, but also a common allergen. Its carcinogenic potential is related to the ability to form nickel carbonyl in the presence of carbon monoxide although carbon monoxide is produced in small amounts during vaping. The core, coil, thick wire and weld joint of the core assembly contain nickel[36]. The content of trace metals in ECLs depends on the device construction. The presence of carcinogenic metals, such as chromium and nickel, is a source of concern about a possible carcinogenic effect as the result of a long-term use of e-cigarettes.
Oxidative Stress And Inflammatory Response
Other potentially toxic flavoring substances commonly used in flavored ECLs are benzyl alcohol and vanillin, ethyl vanillin, menthol, 1-methyl naphthalene, 2-methyl naphthalene, isoquinoline (Table 1)[37]. These flavoring agents can directly impact free radicals generation. E-cigarette vapour contains 1011 free radicals per puff in comparison to classical tobacco smoke containing 1014 [38][39]. It leads to oxidative stress and inflammatory response in the respiratory system. Increased level of neutrophil elastase, proteinase 3, azurocidin 1 and myeloperoxidase has been proved in e-cigarettes users’ sputum[3]. Neutrophil elastase and myeloperoxidase are neutrophil granule enzymes which cause bronchial inflammation and structural damage in diseases, such as cystic fibrosis and COPD (chronic obstructive pulmonary disease). Forming neutrophil extracellular traps (NETs) is also triggered by the constituents of e-cigarettes vapors, such as acrolein[3]. NETs consist of chromatin filaments (neutrophilic DNA) and specific neutrophil granule proteins. NETs formation is a part of neutrophil antibacterial response, and it binds pathogenes. Other mucus proteins, such as deleted in malignant brain tumors 1 (DMBT1) and lysozyme C (LYSC), were decreased in e-cigarette users. DMBT1 and LYSC are the mucosal defense proteins responsible for fighting infections. However, neutrophil cell counts were not increased in the sputum of e-cigarette users, unlike cigarette smokers[3]. Diacetyl, cinnamaldehyde, acetoin, pentanedione, o-vanillin, maltol and coumarin, other flavoring agents, are proved to cause inflammatory response and increase IL-8 secretion mediated by reactive oxygen species generation [37][40].
Table 1
Flavoring compounds commonly used in ECLs.
| Flavoring compounds |
| Acetoin | Diacetyl | Maltol |
| Anisaldehyde | Ethyl vanillin | Menthol |
| Benzyl alcohol | Ethyl maltol | 1-Methyl naphthalene |
| Benzaldehyde | Eugenol | 2-Methyl naphthalene |
| Butyraldehyde | Gingerol | Rheosmin |
| Camphor | Gamma-decalactone | O-Vanillin |
| Cinnamalehyde | Isoamyl acetate | 2,3-Pentanedione |
| Coumarin | Isoquinoline | Terpineol |
| Cyclohexanone | Limonene | Triacetin |
| Cyclotene | Linalool | Trimethylpyrazine |
Pulmonary Irritants
E-cigarette vapor contains numerous substances classified as pulmonary irritants. These are reactive aldehydes such as acrolein, formaldehyde, acetaldehyde [41][42]. Formaldehyde induces irritant response in mice [41]. Electronic cigarettes users are reporting symptoms as cough and dyspnoea, which are the signs of sensory irritation [43]. An animal model study proved the stimulating effect of vaping on the airway nociceptive sensory systems [43]. Inhalation exposure evoked nasal and tracheal sensory irritation in mice [43].
Base components of refill fluids have been found to cause endothelial dysfunction. Inhalation exposure to propylene glycol and vegetable glycerine significantly reduced the sensivity of female mice aorta to acetylocholine [41].
Proinflammatory Cytokines Production
Many authors have proved that vaping may cause inflammatory response in the airway related to producing proinflammatory cytokines [44]. Bronchial epithelial cells and fibroblasts exposed to some flavouring agents (acetoin, diacetyl, ortho-vanillin, maltol) secrete increased amounts of IL-8 [44]. Human lung epithelial cells H292 exposed to e-cigarette vapor intensified IL-6 and IL-8 secretion [45]. Some studies on animal model also indicate correlation between vaping and increased inflammatory markers in blood and bronchoalveolar lavage fluid (BALF). Mouse BALF has been found to contain increased concentration of MCP-1 (potent macrophage chemotactic cytokine) and IL-6 after exposure to e-cigarette vapor [45].
Also e-liquid-dependent suppression of phagocytosis was observed in phagocytic cells. Nicotine itself affects human immune system due to its immunosuppressive effect. Nonetheless, no significant difference in phagocytosis impairment was shown – both nicotine and non-nicotine products cause phagocytosis suppression [46]. Cinnamaldehyde reduces NK cells efficiency (dose-dependent effect) [46]. Those cells are responsible for pathogens and impaired cells elimination. The malfuncion of the immune system may increase susceptibility to respiratory infections.
Mucin Production
Mucin concentration changes were also observed in e-cigarette users[3]. MUC5AC, gel-forming airway mucin, which is associated with COPD progression, in sputum samples of both cigarettes and e-cigarettes users was increased. COPD increases risk of developing lung cancer. Oxidative stress triggered by inflammation is common for both COPD and lung cancer pathogenesis and it presumably may cause long-term effects related to vaping. Also MUC5AC/MUC5B ratio was increased. MUC5AC and MUC5B concentration changes are connected with failed mucus transport in mucoobstructive disease and some other mucus pathologies, such as mucus stasis and mucus obstruction[3]. In vivo studies in animal modelshowed that exposure on e-cigarette vapor consisting of propylene glycol, vegetable glycerin, nicotine (18 mg/ml) and flavoring agent increases mice BAL fluid cellularity and oxidative stress markers. The study also showed increased MUC5AC production, which indicates airway hyperreactivity [3][47].
Respiratory Microbiota And Pulmonary Infections Susceptibility
Recently, changes in the respiratory microbiota (microbial dysbiosis) as a result of vaping are discussed. Exposure to ECLs flavouring agents cause changes in mucin production and immune cells activity in the respiratory tract, which alters airways homeostasis and may disrupt respiratory microbiota [48]. E-cigarette usage increases pneumoccocal (Streptococcus pneumoniae) adhesion to airway cells [49]. Vaping may affect increased susceptibility to pulmonary infections [50]. The latest research has shown a potential impact on e-cigarette users vulnerability to severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection (COVID-19 disease) [51][52][53]. These findings are related to angiotensin-converting enzyme 2 (ACE-2) induction in lungs as a result of vaping. Interestingly, ACE-2 induction in mice was sex-dependent and occured more effectively in males [54]. ACE-2 is an entry receptor for the SARS-CoV-2 due to its role in connecting host cells and SARS-CoV-2 spike protein [55]. ACE-2 expression is lower in males and its reduction with age is also stronger in males than females [56][57]. According to studies using A549 (human adenocarcinoma cell line) nicotine stimulates expression of the ACE-2 gene and ACE-2 protein secretion [58]. Nicotine up-regulates ACE-2 expression, stimulates SARS-CoV-2 replication and enhances viral proteins transcription [58]. Due to these findings, smoking and vaping increase pulmonary infections vulnerability.
{kind=link}