Intracerebral hemorrhages and ARDS
We found an intracerebral hemorrhage in 13.5% of all ARDS patients with a tendency towards higher bleeding rate in COVID-19 patients not reaching statistical significance neither in the whole cohort nor after propensity score matching. To our best knowledge, this is the first study elucidating the risk of intracerebral hemorrhages in COVID-19. So far, only case reports of devastating intracerebral hemorrhages have been published.(10,11)
We can only speculate why the rate of intracerebral hemorrhages is so high in the ARDS collective. For SARS-CoV2, neuroinvasion and neurotropism have been reported and the Coronavirus was isolated from cerebrospinal fluid and brain tissue.(17,18) In a systematic review, long-term cognitive impairment in a collective of mixed ARDS patients was detected in 70-100% patients at hospital discharge and in 20% 5 years after the ARDS.(19) An imaging study revealed cerebral and hippocampal atrophy one year after ARDS compared to healthy controls.(20) Since the rate of intracerebral hemorrhage in our study detected in COVID-19 seems comparable to other ARDS, a more general pathomechanism with cerebral damage due to systemic inflammation might be responsible. Due to the retrospective nature of our study, we cannot determine if intracerebral hemorrhage in ARDS is caused by an embolic event with secondary hemorrhage or if bleedings are caused primarily by neurotropism and local endothelitis.
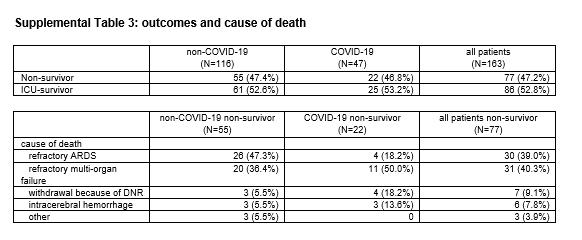
The observed rate of intracerebral hemorrhages during veno-venous ECMO (20.1%; 13/63) therapy matches the rate reported by Fletcher-Sandersjöö et al. 20% (65/351 patients) investigating intracranial hemorrhages during mixed adult ECMO therapy. A systematic literature review suggested incidence of intracranial hemorrhage between 1.8-21% during veno-venous or veno-arterial ECMO. (21,22) ICU survival in our cohort (52.8%) is lower than reported by other data for severe ARDS (38%).(23) Our registry contains severely ill patients as suggested by the predicted mortality of 50.0% according to the SOFA score (24), which might explain these differences.
Anticoagulation during ARDS
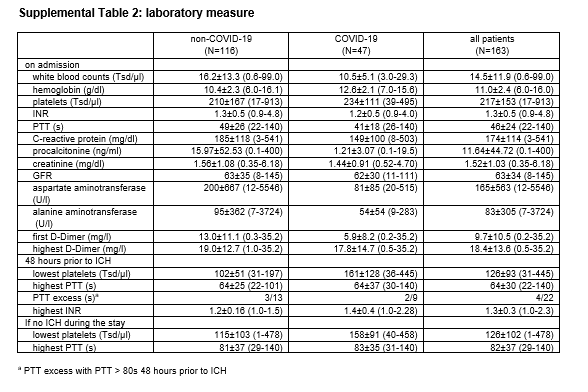
In our registry, 60.1% of all ARDS patients were on anticoagulation other than for prophylaxis of deep vein thrombosis. This might partly explain the high incidence of intracerebral bleeding reported. On the other hand, some phenotypes of pulmonary failure proceed with a hyperinflammatory immune answer, circulatory and subsequent multi-organ failure. The underlying coagulopathy results in clinical complications such as deep vein thrombosis, pulmonary artery thrombosis or clotting on extracorporeal organ replacement therapies. Laboratory measures result in elevated d-dimers, prolonged prothrombin time and thrombocytopenia along with elevated markers for inflammation (c-reactive protein, interleucin 6, ferritin).(25–27) A local reaction such as a virus associated endothelitis or a systemic inflammation might also trigger these prothrombotic events.(2,28)
Limitations:
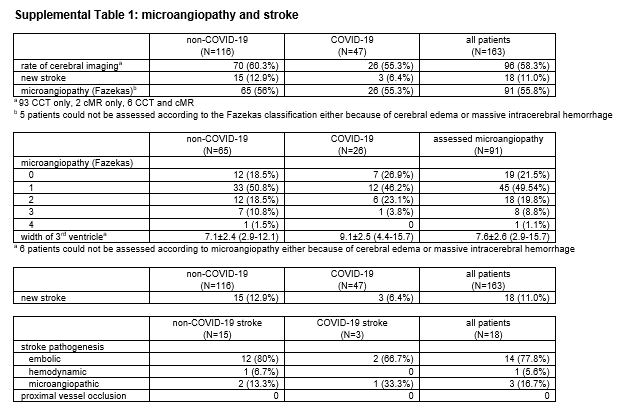
We have to point out several limitations of our study. First, the results of our study are limited in consideration of the small patient numbers. Second, as tertiary treatment center our patients were selected with moderate and severe ARDS as well as high SOFA scores. Results might be different in first and secondary treatment centers. Third, CCT scans were indicated by clinical judgement. It remains unclear how many clinically silent events did occur. Fourth, our anticoagulation regimes under ECMO therapy are empiric for COVID-19 and non-COVID-19 patients and tended to be more aggressive for COVID-19 patients. Fifth, more male patients were in the non-COVID-19 group with male gender being a known factor for intracerebral hemorrhage.(29) In our cohort, we did detected similar bleeding rates in females and males with a tendency towards more bleeding in female patients (19.0% vs 10.5% for females and males, respectively, p=0.153). Finally, the rate of intracerebral hemorrhage in our cohort with 13.5% (22/163) and the rate for strokes of 11.0% (18/163) might not be representative for cohorts in primary and secondary treatment centers with lower SOFA scores and lower rates of organ replacement therapies.
{kind=link}
{kind=link}
{kind=link}
{kind=link}