Patient characteristics in the development cohort
Among the 51 patients selected for this study, after a median follow-up of 48 months from the time of regional lymph node disease, 19 (37%) developed brain metastases while 32 (63%) did not. The characteristics of these 51 patients are summarized in Table 1, comparing patients with brain metastases (Group 3) and patients without (Groups 1 and 2) (Fig.1A).
Each metastatic lymph node was laser-micro-dissected to specifically select a minimum number of 1500 tumour cells, with a mean surface area of 645 000 µm² ± 175 000µm². After RNA extraction, all samples were of good quality, enabling transcriptomic analyses, since the mean RNA integrity number was 8.7 (range 7–10).
The median overall survival calculated from first diagnosis of regional lymph node metastasis was significantly shorter among patients with brain metastases than among patients without brain metastases (39 months vs. 76 months, p<0.01) (Fig. 1B). The median survival from the time of brain metastases was 13.3 months (range 2-72 months). Among patients with BRAFV600E mutation, the median survival was not significantly different for patients with and without brain metastases (14 vs. 17 months).
PROM2 gene expression in metastatic lymph nodes from patients with brain metastases
Transcriptomic analyses were performed on laser-micro-dissected tumour cells obtained from metastatic lymph nodes of the 51 patients. Multivariate analysis was carried out to compare data from patients with brain metastases and those without. Table 2 shows the genes with the highest d-scores and fold-changes, all of them having a Q-value <0.001. We decided to focus on the PROM2 gene, also called prominin-2, with some of the highest d-scores at 4.6 and fold-change of 3.3, and because the PROM2 protein induces membrane protrusions (17) and could thus be implicated in invasive processes.
Using RT-qPCR, we confirmed that the median expression of PROM2 mRNA was significantly higher in metastatic lymph nodes from patients who subsequently developed brain metastases (ΔCt= 4.9, IQR=6.3) than in those from patients who did not (ΔCt= 2.1, IQR=3.9) (p = 0.005, Fig. 2A).
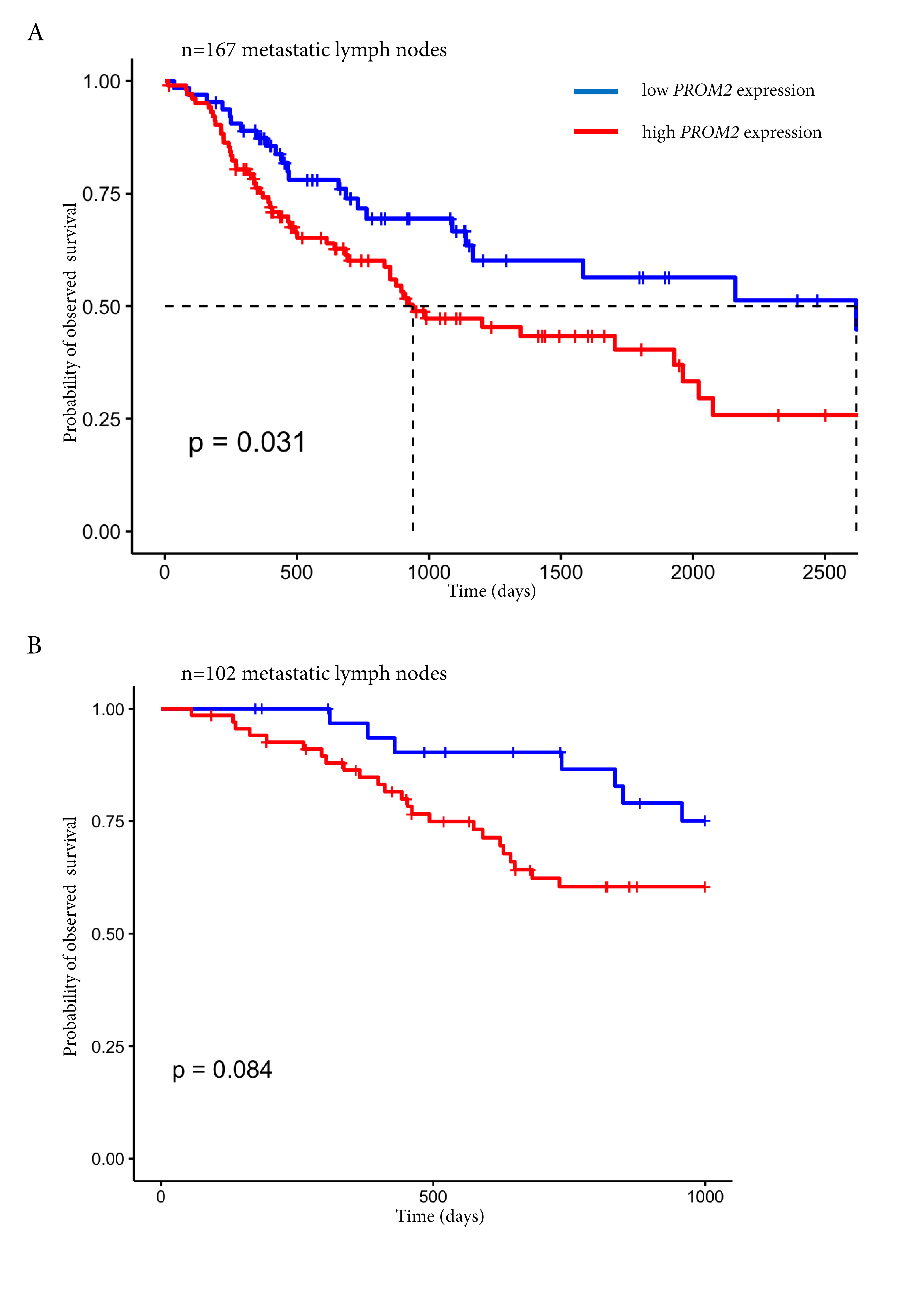
We then analysed transcriptomic data downloaded from public databanks. In 167 metastatic lymph nodes of the TCGA SKCM cohort, a high PROM2 expression was found to be associated with poor survival (p=0.007, score logrank test = 7.15) (Supplementary Fig.2A). In the GSE cohorts that were used to construct Lund molecular classification (GSE22155 and GSE65904) (15, 16), a high PROM2 expression level in 102 metastatic lymph nodes tended to be associated with a poor survival in the first 1000 days of follow-up (score logrank test = 2.99, p=0.08) (Supplementary Fig.2B).
PROM2 protein expression in metastatic lymph nodes is associated with the risk of brain metastases
Using immunohistochemistry, PROM2 expression was assessed on the 51 metastatic lymph nodes. We showed that the PROM2 was only expressed by cancer cells and that the mean “PROM2 IHC score” was significantly higher among patients with brain metastases compared to patients without (8.8 vs. 4, p<0.01) (Fig. 2B).
When we chose a cut-off of 5 for the “PROM2 IHC score”, overall survival was significantly longer among patients who had a score <5 than among patients who reached the cut-off of 5 (p < 0.01, Figure 2C).
Overall, PROM2 expression in metastatic lymph nodes from melanomas is associated with the risk of brain metastases and with decreased survival.
PROM2 expression is low in regional lymph nodes without associated distant metastases
We also compared PROM2 protein expression and overall survival across the three groups, and found that the “PROM2 IHC score” differed gradually and significantly across the 3 groups (Fig. 3B). Overall survival was also much longer for Group 1 with only metastatic regional lymph nodes and without distant metastases after a median follow-up of 80 months (Fig. 3C).
Risk factors for brain metastasis were identified first by univariate analysis and then by multivariate analysis. Using multivariate regression, we identified a “PROM2 IHC score” ≥ 5 and the presence of bone metastases as the two variables significantly associated with the risk of brain metastases. For the “PROM2 IHC score”, the odds ratio was particularly high, at 28.2 (p=0.003, Table 3), showing the strongest association with the risk of developing brain metastases.
Among patients with resectable regional lymph node metastases and stage III melanoma, an elevated “PROM2 IHC score” enabled identification of a high-risk group for distant metastases, including brain metastases.
Validation cohort confirms PROM2 as a biomarker for distant metastasis
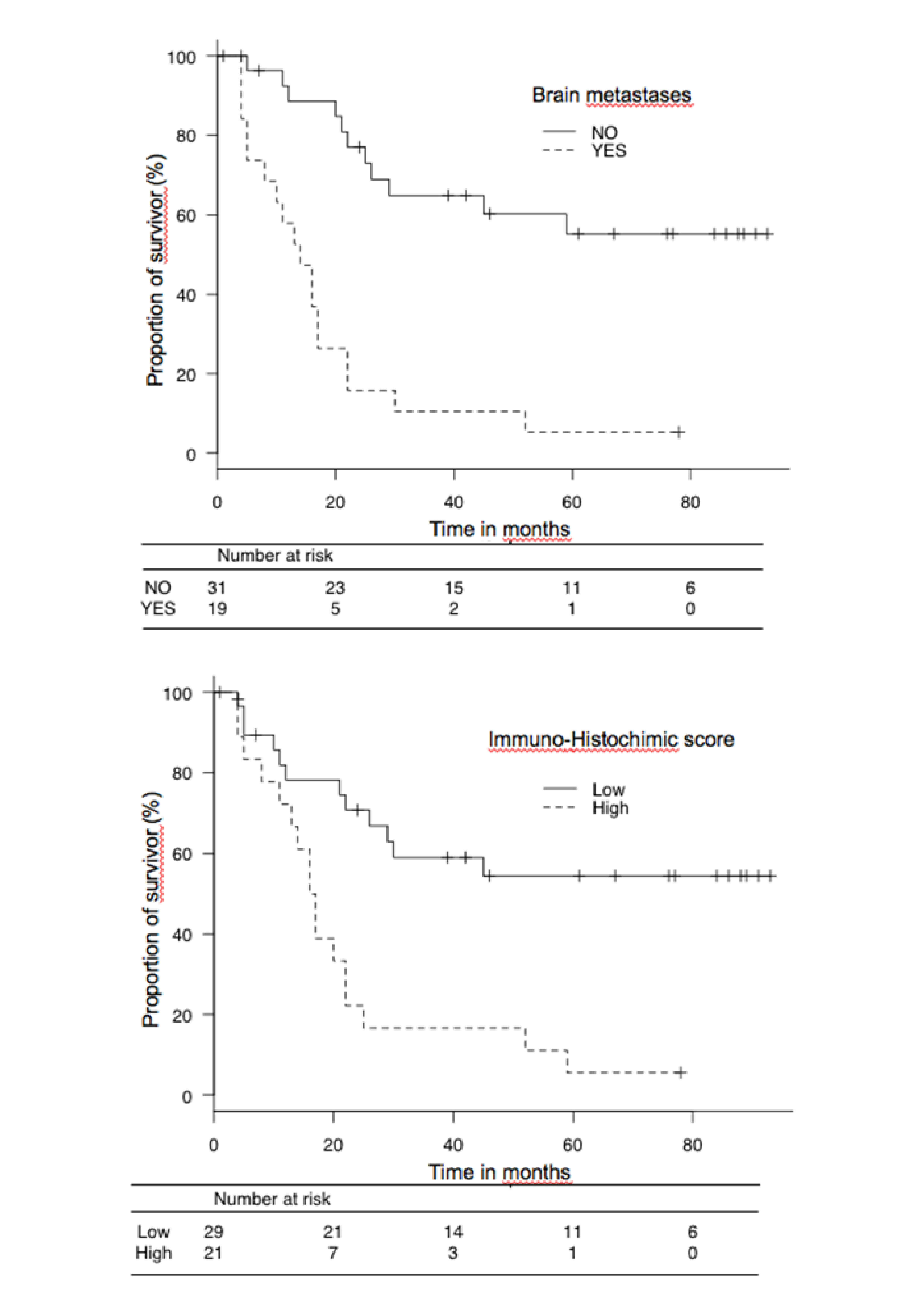
Between 2013 and 2014, 50 additional patients with stage III melanoma at diagnosis and a frozen biopsy sample from lymph node metastases were included in this validation cohort. After a median follow-up of 48 months from the time of the regional lymph node disease, 19 patients (38%) developed brain metastases while 31 (62%) did not. There was no significant difference between the development and the validation cohorts for clinical characteristics or melanoma features (Supplementary Table 1).
In this validation cohort, when PROM2 mRNA expression was assessed on melanoma cancer cells laser-micro-dissected from metastatic lymph nodes, it was significantly higher among patients who developed brain metastases (median ΔCt=5.1, IQR=2.3) than among patients who did not (median ΔCt=2, IQR=4.6) (P < 0.01). The “PROM2 IHC score” was also significantly higher in case of brain metastases (7.4 vs. 2.1, P < 0.01). Using a cut-off of ≥5 for the “PROM2 IHC score” in multivariate regression, the “PROM2 IHC score” was the only factor associated with the risk of brain metastases.
In the two cohorts, in univariate analysis, a high “PROM2 IHC score” ≥5 in metastatic lymph nodes was not associated with the risk of other metastatic sites (lung, liver, bone), except for lung metastases in the validation cohort (Supplementary Table 2).
In both the development and validation cohorts, the presence of brain metastases and a “PROM2 IHC score” of ≥ 5 were the only two factors significantly associated with mortality (Table 4 and Supplementary Figure 3).
{kind=link}
{kind=link}