Post viral anosmia lasting weeks to months has been previously reported in the setting of rhinovirus and human coronavirus infections (1, 2) but in this current pandemic, olfactory dysfunction (OD) has emerged as a common key presenting symptom of COVID-19 infection. Early meta-analysis by Tong et al. (3) of studies published up to 19 April 2020 reported a prevalence of 52.7% of OD among 1627 COVID-19 patients. The associated symptom of loss of taste was also reported in 43.9% of 1390 COVID-19 patients. More recent meta-analysis by Pang et al. (4) examining studies prior to 1 August 2020 demonstrated a pooled frequency of 56% among 17,401 COVID-19 positive patients from 60 studies. The reports of COVID-19 associated OD, led to the United States Centers for Disease Control and Prevention (5) and the World Health Organization (6) including smell and taste dysfunction as early presenting symptoms of COVID-19 infection, and a reason for patients to self-isolate.
Proposed mechanisms of OD in COVID-19 infection include conductive anosmia, damage to olfactory epithelium and direct SARS-CoV-2 virus infection of the olfactory cortex within the central nervous system. Respiratory virus infections including human coronaviruses apart from SARS-CoV-2 can cause nasal oedema or congestion which can impair conductive airflow and thus odorant delivery to olfactory epithelium (2). Temporal correlation has also been found between transient anosmia and upper respiratory tract symptoms such as nasal obstruction in COVID-19 infection (7). More specifically, the olfactory epithelium has been proposed to be the site of nasal infection causing anosmia due to the localisation of SARS-CoV-2 host receptors ACE2 and the protease TMPRSS2 on the sustentacular cells of human and rodent olfactory epithelium (8, 9). Although these receptors are absent on olfactory sensory neurons, evidence towards a central cause for anosmia derives from studies showing hyperintensities within the olfactory bulbs of COVID-19 patients on magnetic resonance imaging (10, 11).
The majority of the present literature on prevalence of OD in COVID-19 infection relies on patient self-reporting. This has resulted in heterogeneity between studies, ranging from study author designed questionnaires relying on patient recall (12) to more formal validated questionnaires such as the Sino-Nasal Outcome Test (SNOT-22) (13). However, Pang et al. found that patient reported symptoms of olfactory dysfunction, although specific (93%), have been found not to be sensitive (48%) for COVID-19 infection (4). In their meta-analysis, pooled frequency of OD in COVID-19 patients was found to be higher in patients assessed by objective olfactory testing (0.76) as compared to subjective surveys (0.53), although admittedly this difference did not amount to statistical significance (p = 0.089).
Subjective reporting of OD in COVID-19 infection may not indicate objective presence of hyposmia or anosmia. Vaira et al. (14) evaluated 345 COVID-19 patients and found that while 225 (65%) of patients self-reported OD during illness, a total of 241 (70%) were found to be objectively hyposmic or anosmic by evaluation with the Connecticut Chemosensory Clinical Research Centre orthonasal olfaction test (CCCRC). Furthermore, of 89 patients who self-reported no smell or taste dysfunction, an additional 30.3% were found to be objectively hyposmic. Conversely, Lechien et al. found that among 78 COVID-19 patients with sudden onset anosmia recruited in Belgium during the early pandemic in April 2020, 87.5% of patients were SARS-CoV-2 viral load positive if they had anosmia < 12 days, and only 24% of all evaluated subjects with self-reported anosmia were objectively found by the “Sniffin’ Sticks” test to actually be normosmic by objective criteria (15).
Validated means of objective evaluation of OD during the COVID-19 pandemic have involved the use of tests such as the CCCRC and “Sniffin’ Sticks” as mentioned above in addition to the University of Pennsylvania Smell Identification Test (UPSIT) (16). These three tests evaluate discrimination between various provided odorants and provide an assessment of the participant’s degree of hyposmia. Olfactory threshold is also assessed using the CCCRC by having subjects attempt to detect increasing dilutions of denatured ethyl-alcohol (17, 18).
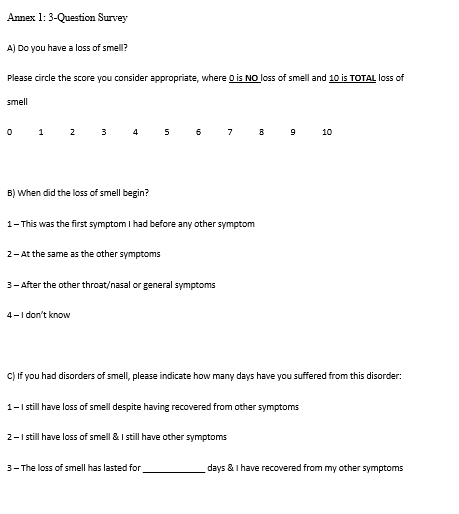
In this study, we describe OD assessment in the inpatient setting of patients both suspected of and with confirmed COVID-19 infection via UPSIT objective assessment and a simple self-reported 3-item questionnaire.
{kind=link}