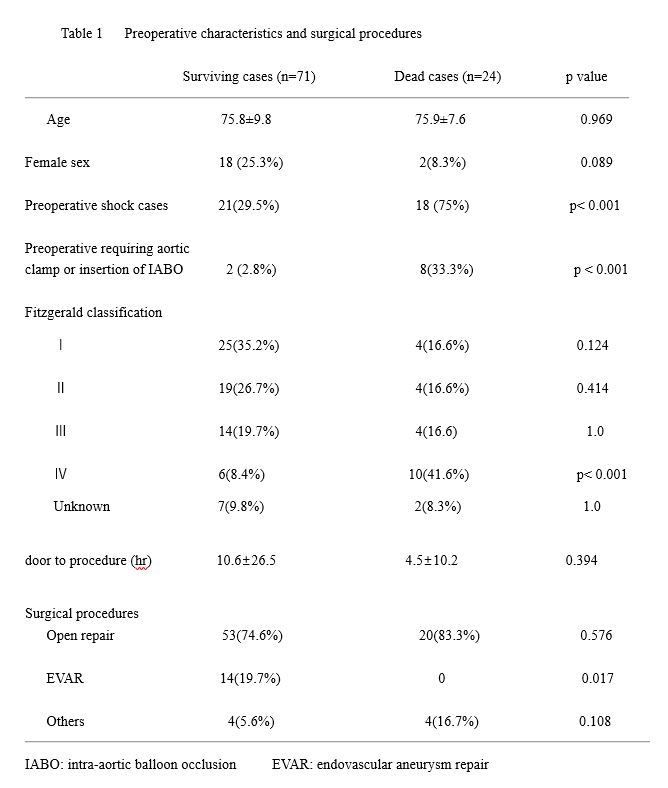
Surgical outcomes for r AAA have improved, but mortality is still high at 20–30% 9),10). In our study, out of 95 cases of r AAA, 24 were dead in hospital and the hospital mortality rate was 25.2%.
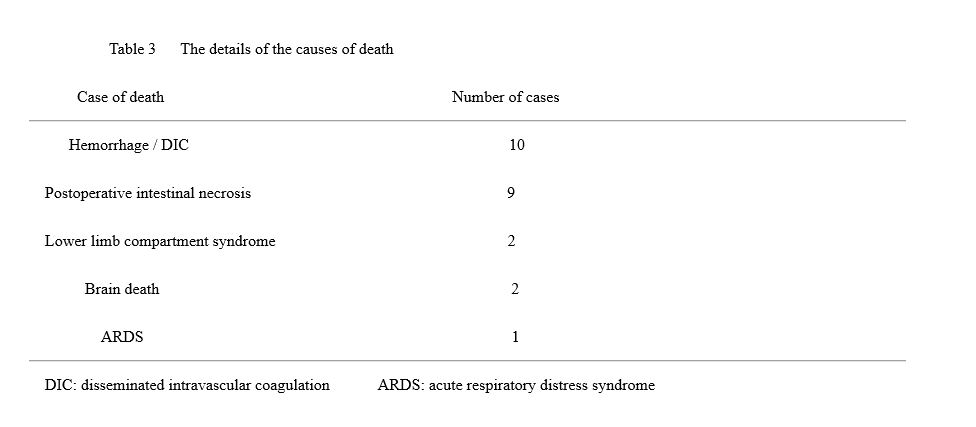
Examining the causes of death in the 24 dead cases, hemorrhage control difficulties and postoperative intestinal necrosis were account for the majority. Therefore, controlling and overcoming both of these may contribute significantly to improve surgical outcomes.
First of all, regarding hemorrhage control, it is important to start of surgery while hemodynamic is stable. In our study, among the dead cases, there were significantly more cases preoperative shock and 7 of the 10 cases who died from DIC or hemorrhage required IABO insertion or aortic clamp by thoracotomy or cardio pulmonary resuscitation (CPR). In other words, if hemodynamics is disrupted, surgical outcomes will deteriorate.
The first touch for r AAA is a vascular surgeon at our hospital. In addition, EVAR is performed by radiologist at our hospital. Therefore, even in cases where EVAR is possible, open repair may have to be selected if there is no time to arrive at the radiologist who performed EVAR.
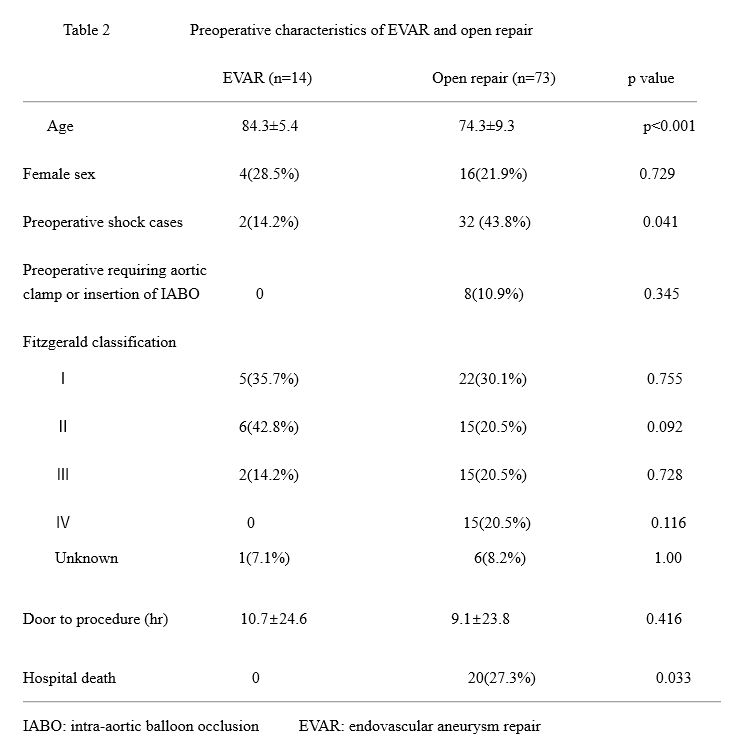
In recent years, it has been reported that EVAR has a better performance as a surgical procedure 1)–5). But comparing EVAR with open repair, there are many preoperative high-risk cases in open repair group. The difference is reflected in the results of mortality and morbidity. Considering the preoperative risk, there is no difference in long-term mortality between EVAR and open repair, or rather, in the high-risk group, EVAR has a higher mortality rate 10). In our study, there were no deaths in the EVAR cases, and all deaths were open repair cases. Mortality was significantly higher in the open repair group than in the EVAR group (0/14 in the EVAR group, 20/73 in the open repair group, p = 0.033). However, among EVAR cases, there were few cases with preoperative shock, and there were no cases requiring aortic clamp by thoracotomy or IABO insertion due to hemodynamic failure. Robinson et al. have made a similar report 10), EVAR does not independently reduce long-term mortality compared with open repair. Furthermore, time from symptom onset to incision and the time from hospital admission to incision were significantly longer for EVAR in comparison to open repair. In our study, there was no difference in door to procedure time between the EVAR group and the open repair group. Looking at the long-term results of EVAR and open repair, there was no difference between the two groups. From the above, we cannot conclude that EVAR is superior to open repair for the treatment of r AAA, the surgical procedure should be selected according to the circumstances of each institution as well as aneurysm anatomy. At our hospital, if it took a long time for the radiologist to arrive at the hospital and EVAR could not be started immediately, we sometimes had no choice but to select open repair.
If hemodynamics disrupted before surgery, it is recommended to perform surgery after aortic clamp by thoracotomy or IABO insertion to stabilize hemodynamics 11),12). Judging from our study, the prognosis is poor if such a hemodynamic failure occurs. IABO is a procedure that is generally used in the trauma area 13), but it should be known as a treatment option even for r AAA. Aortic clamp by thoracotomy and IABO insertion are the last resort, and it is important to start surgery before such a procedure is needed. In other words, the most important thing is how stable the surgery can be started.
Of the 10 cases who required aortic clamp by thoracotomy or IABO insertion due to hemodynamic failure, 2 had IABO insertion and 1 had left thoracotomy aortic clamp at the emergency room. In these three cases, hemodynamic failure occurred before considering the indication for EVAR, so it was necessary to transport them the operating room and open abdomen very quickly. However, all three cases could not be saved. In addition, although he entered the angiography room for the purpose of EVAR, he inserted IABO due to hemodynamic failure, but he abandoned EVAR due to an access route and was rushed to operating room for open repair. However, he could not be saved. Preoperative hemodynamic failure is fatal, and can lead to hemorrhage control difficulties during and after surgery, lead to death.
Regarding surgical procedures after laparotomy, it is important to avoid touching the retroperitoneum where hematoma is detected on preoperative CT scan. In the unlikely event that hematoma ruptures and blood squirts from the rupture hole due to touching retroperitoneum hematoma, an assistant presses the rupture hole to control hemorrhage, a surgen should peel off the area near the renal artery quickly and clamp of abdominal aorta. There is a report that vena cava, left renal vein, left renal artery, pancreaticoduodenal vein, spleen were damaged by aortic clamp 11), so caution is required. There is also a method of controlling hemorrhage by inserting an occlusion balloon into the rupture hole, but care must be taken so that the balloon insertion takes time and hemodynamics breakdown does not occur. In addition, cutting and transection of the left renal vein expands the field of view and reduces unnecessary hemorrhage. We have not experienced any complications due to transection of the left renal vein.
Next, regarding how to prevent postoperative intestinal necrosis, there is a close relationship between ACS and intestinal ischemia, and morbidity and mortality increase when ACS occurs 14)–17). Preoperative hypotension, preoperative consciousness disorder, intraoperative massive bleeding (5L or more), and use of IABO are said to be risk factors for ACS 17),18). Intra-abdominal pressure (IAP) is most easily measured by means of bladder pressure through a urinary catheter. IAP normally runs in the range of 5 to 7 mmHg in critically ill patients 19). Postoperative r AAA may result in an IAP ≧ 12mmHg. In some cases, IAP12mmHg or higher causes organ dysfunction such as decreased renal function. In general, it is said that when it exceeds IAP 20mmHg, it causes organ failure 20). Paty et al.21) suggest that IAP should be measured hourly and decompressive laparotomy should be performed when it exceeds IAP 20mmHg with end-organ dysfunction such a reduced urinary output or ventilator difficulties with peak airway pressure. It has been reported that open abdominal management for ACS prevention reduces intestinal ischemia and excision and improves mortality 22),23). We are also actively introducing open abdominal management for ACS prevention for the last few years. Five out of 10 cases were saved, and if they survive the acute phase, they will be hospitalized for a long time, but there is a high possibility that they will be saved. Acosta et al. 23) reported that the management of open abdomen at the time of the first surgery has a better prognosis than the management of open abdomen in the second term. Even if abdominal wall can be closed, our policy is to not force the abdominal wall to close in consideration of the risk factors of ACS mentioned above. If necessary, we will actively do open abdominal management. There is also a report that it should be noted that the diagnosis of ACS may be delayed in EVAR cases 24). By avoiding ACS, intestinal ischemia/necrosis can be prevented and the mortality rate can be reduced. For that purpose, it is necessary to do open abdominal management without hesitation. Open abdominal management requires long-term hospitalization and strict systemic management. Not only infection control and nutritional management, but also a close relationship with the gastrointestinal surgeon is important. IAP should be measured, be careful with ACS. The intestinal tract status should be monitored, and if necessary, intestinal resection and closing abdominal wall should be performed at an appropriate time.
Figure 2 shows yearly changes in abdominal aortic aneurysm surgical procedure at our hospital, including elective surgery and emergency surgery. Recently, the number of full-time radiologist at our hospital has been increased. Therefore, in the future, EVAR may increase as a surgical procedure for r AAA. If this happens, it will be necessary to observe in the future whether or not the surgical outcome will improve compared to now.
{kind=link}
{kind=link}
{kind=link}