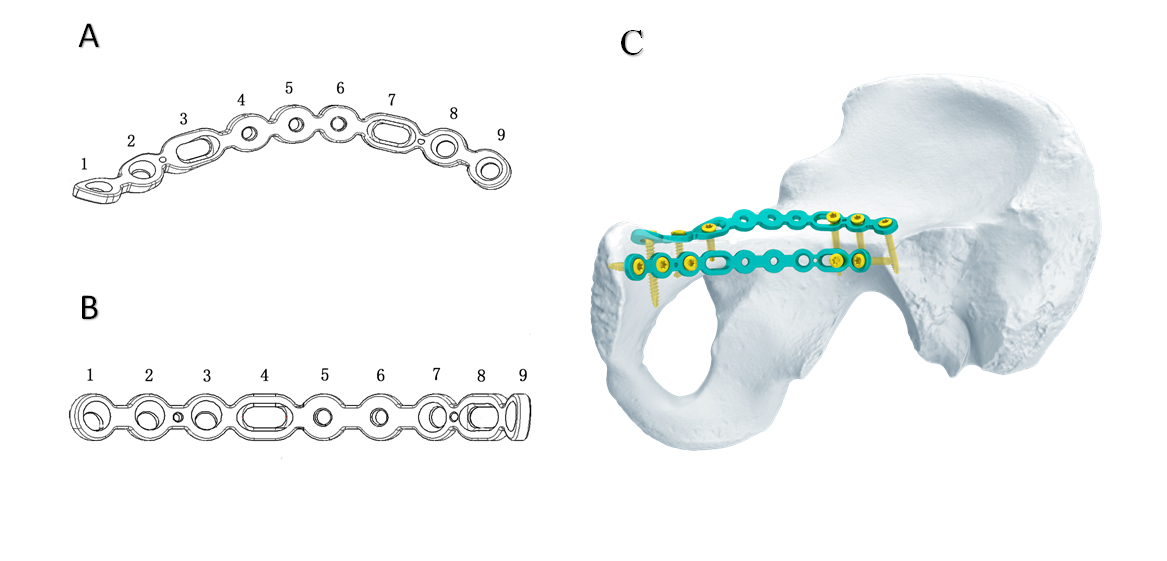
Extensive surgical approach for acetabular fractures is often accompanied by the possibility of perioperative complications such as infection, blood loss and neurovascular damage (3, 21). Although closed reduction and minimally invasive surgery decrease surgical complications, but it is difficult to achieve anatomical reduction of articular surface (10). The limited pararectus approach we used did not dissect the spermatic cord (or round ligament) and extra-iliac vascular nerve bundle, thereby reducing the risk of iatrogenic neurovascular injuries and complications. And it helped to achieve good reduction quality and functional results. Since it is located in the lateral margin of the rectus abdominis, the exposure of the anterior wall and quadrilateral plate will not be blocked by the rectus abdominis as happened in the modified Stoppa approach (22, 23). We believe that direct and adequate exposure of fractures is instrumental in achieving anatomical reduction. On the other hand, owing to the limitation of minimally invasive incision, it is difficult and time-consuming to remodel the plate intraoperatively. The anatomical plate in this study is designed according to the physiological anatomical morphology, which makes it has good congruity to the irregular pelvis and has the function of auxiliary reduction (Fig. 4) (17).
The average operative time and blood loss were less than that of extensive surgical approach. Keel reported that the average operative time and the mean blood loss of the pararectus approach were 197 min and 1700 ml, respectively (3). Using the modified Stoppa approach described by Sagi the operation time and blood loss were 263 min and 750 ml, respectively (16). While by using an oblique mini-incision, Farouk (10) reported an average blood loss of 110 ml and an average operating time of 95 min. In our case series, the mean blood loss of 334.1 ml is more than Farouk `s, but significantly less than that of the established procedures published previously (1-3, 5). Moreover, average operative time of 90.9 min in our sample, which is comparable to Farouk `s study. The wound of the limited pararectus approach is very small which may be the main reason for lower blood loss.
We consider that standardized image reading ensures rigorous evaluation of surgical reduction. On postoperative CT scans, the mean residual gap and step displacement was 2.9 mm and 0.7 mm, respectively. The anatomical and imperfect reduction rate was 94.1%. The functional outcome at the last follow-up were graded as good and excellent in 88.2% patients. The clinical result is comparable to the previous research (1, 3, 15, 16, 24). Good radiological and clinical results are derived from the adequate visualization of fracture sites and valid fixation of the anatomical plates.
Traditionally, the suprapectineal and infrapectineal plates which are used to fix the anterior column and quadrilateral plate are usually inserted using the standard ilioinguinal and modified Stoppa approaches. The good congruity of the plate is obtained by reshaping the reconstruction plate intraoperatively. Owing to the limitation of the minimal incision in our study, the bone surface was not exposed fully, which made it difficult and time-consuming to reshape plate during operation. In recent years, some new anatomic plates instead of conventional reconstruction plate have been used for buttress and span fixation of the quadrilateral plate and medial surface of the posterior column (17, 25). The anatomic plates have good biomechanical properties and congruity with the irregular acetabulum surface, which make the fixation more valid and easier. Moreover, in this study, we observed that the displacement between the fragment and the intact part was further reduced as the lag screw was inserted into the plate. Nevertheless, the relatively simple type of fractures in our cases facilitates the reduction, fixation and clinical outcome too. We consider that strict selection of patients is the key to ensure good surgical results, especially when using minimally invasive approaches.
The relative minimally invasive pararectus and modified Stoppa approaches are also accompanied with incidence of surgery-related complications ranging from 10.7% to 45.4% (13, 26). It is easy to understand that extensive dissection of the neurovascular bundle and inguinal canal and intraoperative overstretching are supposed to be the main causes of surgical complications. The limited pararectus approach passes through the soft tissue space between the rectus abdominis and the neurovascular bundles to obtain closer access to anterior wall, anterior column and quadrilateral plate of the acetabulum. In this area, the extraperitoneal reflexed spermatic cord is the major obstacle of surgical exposure, pulling outward may be the cause of peritoneal rupture which occurred in one of our case. However, Both the wound and fracture were healed rapidly during follow-up, and no wound infection, fat liquefaction, ectopic ossification, or secondary displacement was recorded.
Closed reduction of displaced acetabular fractures may be minimally invasive, but finger palpation blindly for fracture manipulation and assessment of reduction may be inaccurate and may result in miss diagnosis of rotational displacement and more radiation exposure of medical staff (10). However, in this study, the mini-pararectus approach might be a good choice for certain types of acetabular fractures involving low anterior column and quadrilateral plate, including anterior wall, anterior column with quadrilateral plate, simple transverse and anterior column with posterior hemitransverse fractures without iliac fragment. It can provide direct view through the soft tissue space, which decreases the risk of neurovascular injury and is beneficial to achieve anatomical reduction.
There are several limitations to this study. First, it is required to extend the minimal incision to the standard pararectus approach for the treatment of high anterior column fractures involving iliac wing and dome fragments in the elderly, which may be the main disadvantage of this approach. Besides, the minimal approach might not be suitable for delayed cases, patients with obesity or lower abdominal surgery history. Besides, we think the current problems of the two plates mainly include: (1) the length and model are invariable, so it is difficult to completely fix a long pelvic brim fracture; (2) the plasticity is not as good as that of stainless steel reconstruction plate, and excessive shaping will reduce the strength of the plate. This is a preliminary study on the use of the limited pararectus approach for the treatment of acetabular fractures. A prospective comparative study involving more cases needs to be further carried out, and long-term follow-up of patients is needed to be performed in the future.


{kind=link}