This is the first published report in the medical literature that study a new approach to decrease neurovascular bundle toxicity and improve quality of life for patients with prostate cancer treated with radical brachytherapy as monotherapy. Transperineal HA injection on the side of the prostate into the lateral aspect of the prostate fat was used to consistently displace several autonomic fibres (afferent and efferent) and vessels the lateral wall of the prostate away from the effective and biologic life of radiation sources. In low and low-intermediate risk patients treated with HDR monotherapy, the HA injection was administered before dose delivery for HDR patients. This study was approved by the institutional ethics committee and all patients signed informed consent.
Sexual function
The sympathetic and parasympathetic nervous system both play an important role in sexual function. Sacral parasympathetic fibres from S2–4 travelling through the pelvic plexus and forming the nervi erigentes dorsolateral to the bladder and prostate are responsible for the blood flow into the corpora cavernosa resulting in penile erection. Sympathetic fibres are responsible for emission of semen from the seminal vesicles into the prostatic urethra and antegrade ejaculation. Thus, iatrogenic damage to the parasympathetic and sympathetic pathways during radical brachytherapy may result in erectile and ejaculation dysfunction [10,11].
Study model
The injection of HA is performed before needle placement creating a minimum of a 1.5-2 cm space between the prostate capsule and neurovascular bundle. Having finished the HDR brachytherapy needle placement and before dose delivery, microMOSFET detectors are placed within the prostatic capsule and in neurovascular bundle. Intraoperative trans-rectal ultrasound (TRUS) is used for verification of the microMOSFET placement. In this fashion, we measure the delivered dose to both critical organs during the treatment “in vivo”.
Magnetic Resonance pre and post-implant imaging are used to assess the dimensions of the new space create.
The patient received one implant and one fraction of HDR. Fraction dose was 22 Gy.
Brachytherapy procedures were done under spinal anesthesia. The needles were positioned by transperineal placement under real time TRUS guidance using a template. Axial cross-sections were captured in 5mm steps and transferred to the Treatment Planning Software. Prostate gland, normal structures (urethra and rectum) and needle positions were identified and mapped based on the ultrasound image. Dose optimization was done on the reconstructed applicator geometry using dose point and manual optimization algorithms to determine dwell positions and times.
The prostate without safety margins was then defined as the planning target volume (PTV) to be treated with the prescribed dose (PD). Based on the dose volume histograms (DVH) data, the quality of plans and implants was evaluated using following indicators:
- The rectal dose was calculated at the anterior edge of the TRUS probe and was limited to ≤ 75% of the prescription dose.
- The dose to any segment of the urethra was limited to ≤ 110% of the prescription dose. V120 and D100 of the prostatic urethra were determined (volume that received a dose of 120% and dose delivered to 100% of the urethra).
- The PTV V90, V100, V150 and V200 (% of PTV receiving 90%, 100%, 150% and 200% of the PD) were recorded.
- D90 (dose delivered to 90% of the PTV) was calculated.
All patients are discharged from the center on the same day of the procedure between 6-8 hours of implantation.
Technique of hyaluronic acid injection
The injection of HA is performed before needle placement. Based on our experience of rectal protection with HA in prostate cancer Brachytherapy [12, 13]. Below we describe the technique.
Step 1: The TRUS probe with the transperineal template is placed and fixed in the standard fashion. Magnetic Resonance pre-implant imaging are fused with the intraoperative TRUS image. Then all treatment needles are placed under TRUS guidance.
Step 2: Using TRUS guidance, an additional needle is placed guiding the needle tip into the peri-prostatic fat, between the lateral prostate capsule (treated volume) and the neurovascular bundle, at the level of the maximum transverse diameter of the prostate (reference level). Under direct TRUS guidance, the needle tip is advanced to the level of the seminal vesicles and then to the level of the prostatic apex. Extreme care is taken not to perforate the prostate capsule with the needle tip.
Step 3: The additional needle is connected to the syringe containing HA. After aspirating to ensure that contact with a vessel had not occurred, between 6 and 10 cc of HA is injected within lateral prostate capsule and the neurovascular bundle. This is performed under continuous TRUS guidance to view and verify the new space created by the injection. The total injected amount is related to the need for systematically creating a minimum of a 1.5-cm space between the prostate, seminal vesicles, apex and neurovascular bundle throughout this length.
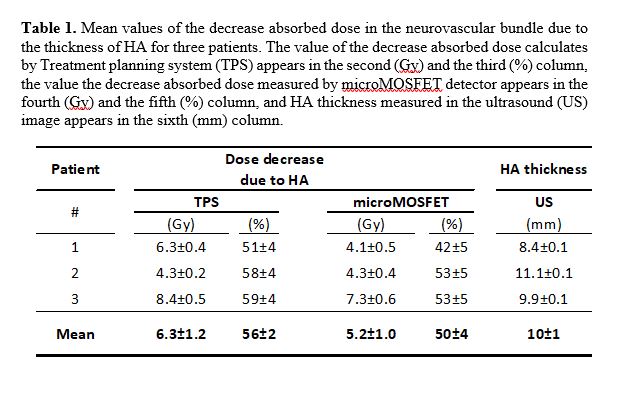
Step 4: Under TRUS guidance, the neurovascular and lateral prostatic catheters with the microMOSFET are placed. The absorbed dose is calculated as the difference of the dose values between the points separated by the HA. We calculated the value of this decrease using the Oncentra Prostate planning system of Nucletron, and measuremed this value using TN-502-RDM MOSFET detectors, hereafter microMOSFETs, manufactured by Best Medical Canada (Ottawa, Canada).
The dimensions of microMOSFET detectors enabling their insertion in needles used for HDR brachytherapy. Detector response in voltage is measured before and immediately after each exposure or treatment completed. The voltage difference between these measurements is proportional to the absorbed dose, which is obtained by applying a pre-determined calibration factor (CF) in Gy/V. In the clinical setting, these detectors are inserted in additional needles to those used in the treatment, placed at both ends of the HA thickness, allowing measurement of the true dose delivered. After correct insertion of the tip of the needle, monitored by US, the detector is placed in the end. In these conditions, the position of the sensitive part of the microMOSFET is approximately to 8 mm from the tip of the needle. The measurement system includes a mobile MOSFET Reader TN-RD-16 electrometer that can simultaneously measure up to five detectors.
In the same plane of the ultrasound image in which the two microMOSFET are placed, and in the two points marked by the needles in which the detectors are for each patient, the absorbed dose is calculated with the Treatment planning system (TPS) once the planning of the treatment has completed. In this way we can compare the value of the decrease absorbed dose obtained by both the TPS and the microMOSFET.
The microMOSFET was calibrated employed a water phantom. The absorbed dose for calibration at the measurement was 1 Gy, the source-detector calibration distance was 3 cm, and the dwell time required for this absorbed dose value at the calibration point was determined using the Oncentra Prostate planning system. The CF for twenty microMOSFET detector was obtained, taking five consecutive measurements for each, to calculate its reproducibility.
All measurements and treatments were performed using Flexitron afterloader and the 192Ir V2r source (Nucletron/Elekta, Stockholm, Sweden).
Step 5: After the HDR treatment is completed, both catheters containing the microMOSFET detectors are removed for reading.
Uncertainties
We considered two groups of uncertainties, those associated with dose calculation by the TPS and those related to dose measure by microMOSFET detector [14, 15]. For uncertainties of calculated absorbed dose, we considered source intensity (Air kerma strength, SK) and the interpolation associated with the TPS. For uncertainties of measured absorbed dose, uncertainty related to the global CF corresponding to each detector, we consider in addition to the previous uncertainties, the source-detector calibration distance, the electrometer resolution and the reproducibility.
Hyaluronic acid
The HA is a polysaccharide normally found in human tissues as a component of the connective tissue and it has an absorption coefficient equal to water. Normally, it plays a vital role on the skin and in the synovial fluid of the joints. It is normally degradable by the normal enzymatic system in relative short time. However, to make it last for months when used for the treatment of skin wrinkles and osteoarthritis, the compound is modified making it stable for a duration close to 1 year before it is reabsorbed by the body [16, 17]. Only one type of HA is used in this trial.
{kind=link}