HER-3 protein levels in adeno-NSCLC and mechanism of overexpression
Reports of the incidence of HER-3 protein overexpression in NSCLC vary greatly according to the cohort. Previous groups have reported rates of 6.5% (NSCLC) (40), 15.9% (advanced adeno-NSCLC) (27), 35% (EGFR mutant NSCLC) (41), 64% (stage 1 NSCCL) (42), 85.1% (resected stage I-IIIA adeno-NSCLC) (43) and 86.1% (resected stage 0 and 1A1 adeno-NSCLC) (44). IHC methods and scoring have not been previously standardised. Our data uses a validated and robust scoring system based on optical density and H-score. Although our patient cohort is small, we demonstrate that overexpression of HER-3 protein is common in advanced adeno-NSCLC, occurring in over 40% of patients.
The rate of ERBB3 gene amplification in NSCLC is low. The Cancer Genome Atlas Research Group sequenced 230 cases of lung adenocarcinoma and did not identify any ERBB3 amplification (45). The cBioportal and GENIE data sets report amplification in just over 1% frequency (38). A smaller series of 71 cases reported a 1% amplification rate in lung adenocarcinoma (34). In a series of 82 NSCLC patients HER-3 amplification was identified in 26.8% of patients who were treated with the EGFR TKI gefitinib. ERBB3 amplification was more common in those with ERBB2 gain (p = 0.055) and EGFR gain (p = 0.06) but not with EGFR mutations (p = 0.17) (46). It was not possible to perform ERBB3 PCR on all cases in our cohort as tumour tissue was limited, but a sample of 27 cases had sufficient tumour sample to pass quality control. There appeared to be clustering of HER-3 overexpressing cases in those with ERBB3 copy number gain but this does not account for the majority of HER-3 overexpression.
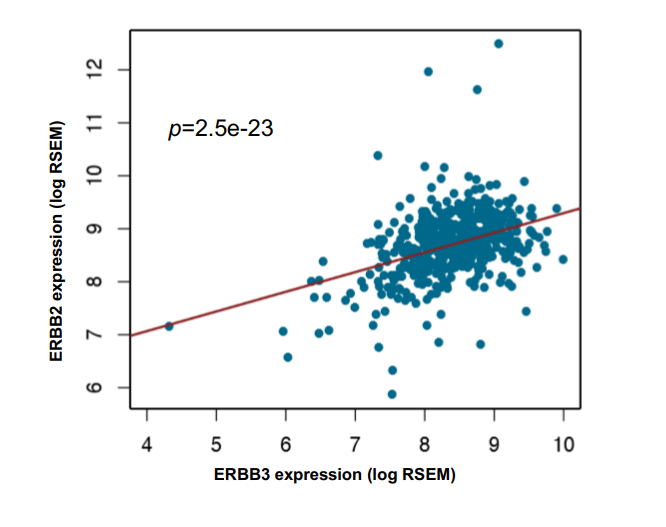
Bioinformatic analysis of large, publicly available datasets allows testing of hypotheses. We interrogated the PanCancer TCGA data set of adeno-NSCLC samples. This dataset includes transcriptome (RNA) and genomic (DNA) data. The genomic data supports our finding of low levels of ERBB3 amplification, which was the most common cause of ERBB3 genetic alteration. It also provided the confirmation that ERBB3 copy number alteration highly associates with its gene expression.
The MEK activity score is an 18 gene signature derived from an experiment to test a mixed-tumour response to the MEK inhibitor, selumetinib. The MEK activity score is a surrogate marker of MEK pathway activation. It is not specific for activation through the HER-3 channel as the MEK pathway is also initiated upon HER-2, EGFR and other receptor activation. It also does not take into account HER-3 downstream activation via the PIK3A/AKT/mTOR pathway. However, as HER-3 activity is predominantly via HER-2/HER-3 and EGFR/HER-3 hetero-dimerisation, we inferred that the MEK activity score could be used as a surrogate of, but not specific to, HER-3 protein expression. If a key node in the HER-3 pathway is found to correlate with MEK activity score it can be concluded that, in that cohort, the node may play a key part in pathway. The lack of correlation with ERBB3 ligands (NRG 1 and 2) expression is an important negative finding. RNF41 also had a significant positive correlation with MEK activity score. This is difficult to interpret given the fact that an increase in a degradation protein would be expected to correlate with a lower target protein level.
In conclusion, HER-3 protein is common in adeno-NSCLC, amplification levels of ERBB3 are low and on TCGA analysis the mechanism of HER-3 protein overexpression does not appear to be ERBB3 ligand dependent. Further investigation is required to elucidate the mechanism of HER-3 protein overexpression in adeno-NSCLC.
HER-3 expression as a prognostic marker
Yi et al26 demonstrated that HER-3 overexpression is associated with a poor prognosis in a cohort of 443 patients with advanced NSCLC (27). The median overall survival in our study was not significantly different between the HER-3 negative and positive patient group. This phase 1 patient cohort may not be truly reflective of the broader population of NSCLC patients, as these patients tend to be fitter with fewer or no co-morbidities.
HER-3 in relation to oncogenic drivers in adeno-NSCLC
HER-2 protein overexpression is reported in 6–30% of patients with lung cancer, which in keeping with our results (47) (48) (49). HER-2 expression is less frequently observed in NSCLC than HER-3 expression. There was some overlap, though no statistically significant association between, HER-3 expression with HER-2 expression or KRAS and EGFR mutations. Previous data have demonstrated that HER-3 plays a role in EGFR TKI resistance. Half of the cases in this cohort with EGFR mutation also co-expressed HER-3. No difference in overall survival was seen between HER-3 expressing and non-expressing groups in the EGFR-mutant cases in this cohort though patient numbers were small.
We therefore conclude that HER-3 represents a common target in NSCLC independent of KRAS and EGFR mutations. We have a simple tool in the form of IHC that can be used to “pre-screen” and stratify patients to receive such HER-3 targeting compounds. Furthermore, there are some patients in which HER-3 expression occurs concurrently with driver mutations and the role of HER-3 in these groups, including in drug resistance, requires further investigation. The relationship between HER-3 expression and other drivers in NSCLC (such as ROS, ALK, NTRK and RET) is yet to be determined.
HER-3 and functional activity in adeno-NSCLC
In the TCGA dataset MEK activity score was associated with EGFR and AREG (EGFR ligand) gene expression. This suggests that signalling via EGFR is key to the oncogenic behaviour in lung cancer. EGFR has been previously reported as a key driver of oncogenesis in lung (and other) cancers (50). Although our initial analysis did not show correlation of ERBB3 with MEK signature, we stratified ERBB3 expression into two groups; “expression low” and “expression high”; and analysed this along with EGFR gene expression. In the ERBB3 expression high group, ERBB3 RNA expression levels positively correlated with MEK activity score but not in the expression low group. The expression of EGFR correlated with MEK activity score in the ERBB3 expression low group. This supports the hypothesis that HER-3 is an alternative pathway for MEK activation in the HER-3 expression high group. This analysis implies a degree of functional downstream pathway signalling via HER-3. In effect, this suggests that when EGFR drives the cancer, the effect of HER-3 is minimal as EGFR drives the downstream signalling. However, as HER-3 expression increases this becomes the main driver of pathway activation. This finding has relevance in terms of proposing HER-3 as a viable drug target in adeno-NSCLC. As a membrane target HER-3 can be potentially targeted with drugs such as HER-3 target antibody drug conjugates in which expression on the surface is key to activity. However, a degree of functional MEK pathway activation suggests that in some patients drugs that rely on abrogation of signalling (such as HER-3/ HER-2 dimerisation drugs) can also be attempted. The challenge in this patient cohort is to predict patients in which this approach will be effective, our data relies on gene expression but transcriptome analysis is complex in a clinical trial setting.
{kind=link}