This study has been the first to examine risk factors related to LF and MDA participation in Myanmar. It assessed three outcomes in an area with ongoing transmission after six rounds of MDA including: persistent infection (measured by CFA), never having taken MDA medication and LF-related hydrocoele. It found that persistent infection was related to both baseline (pre-MDA) factors and low uptake of MDA medication. Never taking MDA medication, in turn, was associated with both program reach and individual compliance factors. Finally, LF-related hydrocoele was significantly associated with increasing age and residing in the historically endemic township of Amarapura.
Despite six rounds of MDA, infection remained significantly associated with baseline risk factors, which include host characteristics and exposure to infected vectors. The relationship between infection and increasing age found in this study is well established.[15] It is thought to relate to both increasing exposure to infected mosquitoes with age and the inefficient transmission of L3 larval stages from mosquitoes to humans.[16]
The higher prevalence of LF infection amongst males found here is also well documented.[15, 17] Historically, it was suggested that this was the result of greater occupational exposure. However, the persistence of male predominance, following adjustment for occupation, outdoor-work and MDA participation in this analysis, supports the hypothesis that there is also a biological basis for this difference.[18–20]
Risk of infection was strongly associated with the number of people per household room, a marker of crowding. Entomological studies have shown that rooms with more inhabitants have an increased density of indoor Culex mosquitoes.[21] It is therefore hypothesised that crowding may lead to greater density of indoor Culex mosquitoes increasing transmission risk amongst household members. Efforts to reduce overcrowding, which are employed for other communicable diseases, may therefore also decrease LF transmission. Whilst a relationship between crowding and infection has not previously been documented, a link has been observed between household size and infection in children in Brazil, where Culex is also the vector.[22] When crowding was replaced by household size in our final model, there was a positive association, but it did not reach significance (p = 0.058, results not shown). This suggests that household size, as well as density, may predispose to infection in Culex regions, but this requires further investigation.
The absence of screens or glass on household windows was also associated with higher infection risk but lost significance following adjustment for survey design. This may be due to sample heterogeneity, and that Amarapura Township had both a high infection prevalence and low number of screens/glass on windows. The relationship is nonetheless noteworthy, because studies in Africa have shown that windows and doors are the preferred entry point for Culex mosquitoes, and the addition of screens reduces their indoor density.[23, 24] Other variables related to night-time vector exposure, including bed-net ownership and usage, also showed a protective association, but did not reach significance. This was probably because bed-net ownership and usage were uniformly high across the study area. Together, this suggests that individuals may have been infected whilst in their household but outside of their bed-net. The addition of screens to household windows could therefore be an effective intervention to reduce the LF transmission and deserves further study and trials.
An interesting finding was the association between small changes in elevation and infection risk. Whilst a negative association between elevation and infection risk is well documented, this typically occurs with larger variations in altitude.[25, 26] This is because at higher altitudes, atmospheric temperatures decrease, resulting in reduced mosquito survival and slower parasite development within the vector.[27] In this area, which is located within the central plains of Myanmar, altitude only ranged between 45 and 269 metres above sea level. This would be insufficient to affect vector survival, but instead, indicates low-lying households that may be closer to bodies of water. The distance from households to large bodies of water was also directly measured. Whilst significant in the univariate analysis, the variable lost significance when it replaced or was added alongside elevation in the final model. This could be because elevation more accurately captured subtle proximity to water such as smaller waterways, areas prone to flooding, or households closest to water along a riverbank. These findings support earlier work in demonstrating the usefulness of elevation as an indirect marker for proximity to water and therefore infection risk in low-lying contexts.[28]
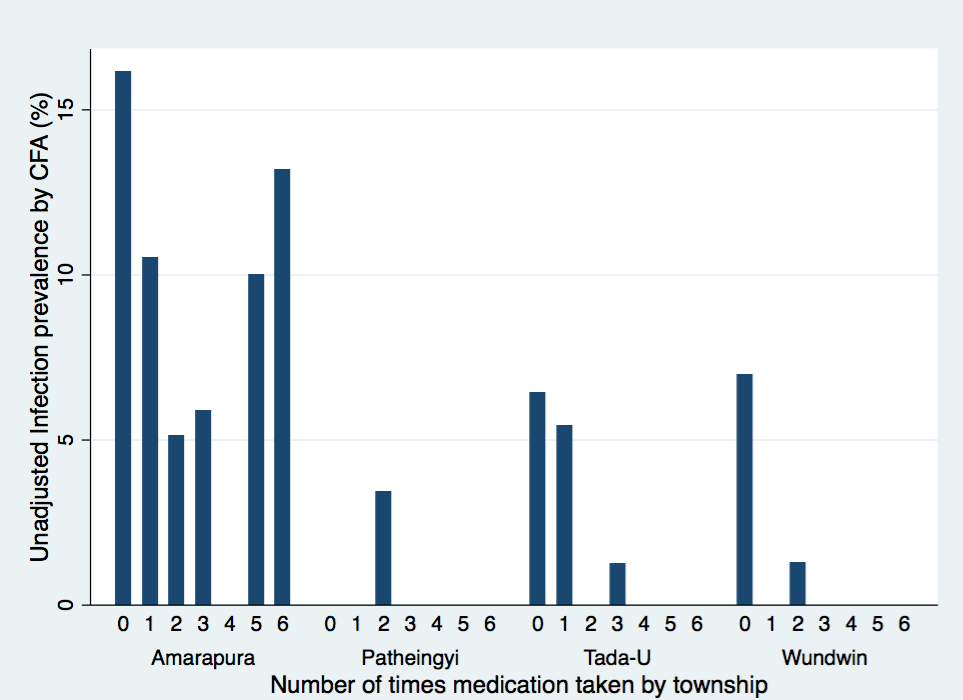
A significant finding in this study was the strong association between persistent infection and never taking MDA. Whilst the relationship lost significance after adjustment, possibly due to the clustering of non-participation, it retained a strong positive effect (OR 2.09). This relationship is explained by both the mechanisms with which MDA medications control LF at the individual and community levels. The predominant effect of MDA is microfilaricidal, thereby reducing local transmission and the chance of new infection.[29] This is reflected in the study area, where villages with greater than 65 percent MDA participation, had a mean CFA prevalence of 2.08%, compared to 9.76% in villages with lesser participation. The secondary effect is macrofilaricidal, reducing the burden of adult worms and therefore eventually CFA.[30] At the individual level, this explains the lower weighted and adjusted prevalence in those who had participated in the MDA program (1.60%) compared to those who had not (6.74%). The high prevalence of infection amongst ‘systematic non-takers’ supports studies elsewhere in highlighting their significant role as a reservoir for ongoing transmission in the community.[31, 32]
Understanding the causes of MDA non-participation, especially systematic non-taking, are therefore crucial to improving control efforts. In the study area, non-participation was related to both programmatic reach (the proportion of targeted persons who are offered medication) and individual compliance (the proportion who take the offered medication).
The programmatic factors associated with non-participation suggest households were either not visited by the program, or the members of the household were absent at the time of the visit. While almost all (95%) of surveyed households reported being visited by the MDA program at least once, the mean number of visits was only 2.59, with fewer visits predictive of never having taken MDA. In the households that were visited, absenteeism further predisposed to non-participation. The likelihood of never taking MDA was lower in persons from households with fewer members present during the last round, and in persons that had migrated from another village. The lower medication uptake in males may also have related to absenteeism, since we found that during daytime data collection men were often away working.
These findings corroborate those of Linn et al. who recently conducted a qualitative survey on barriers to MDA participation in Myanmar (unpublished).[33] They interviewed members of the community and National Program to Eliminate LF (NPELF) in three townships with persistent transmission in Mandalay, and the adjacent Magway and Sagaing Regions. They found community members were often unaware of previous rounds, suggesting they may have been missed. Of those who were aware of the previous rounds, a number stated they had not received medication because they were away. Meanwhile drug distributors reported that financial, human resource and time limitations prevented them from fulfilling their duties and mopping-up recipients who were initially missed. The NPELF should therefore ensure that future rounds reach all households, are sufficiently resourced and conducted at a time when household members are likely to be present. A strong emphasis should also be made to mop-up eligible recipients who were missed during the initial round.
In addition to programmatic reach, our results indicate that individual compliance was a contributing factor to overall MDA uptake. The strong association between ever declining medication and systematic non-participation suggests that a significant proportion of non-participators were offered medication but did not take it. The most common reasons reported in both our study and Linn et al. were fear of side effects or a perception that co-morbidities were a contraindication.[33] Although adverse events are rare, community concern has hampered MDA in many countries and resulted in the postponement of the 2006 MDA round in Mandalay Region.[3] The lower participation in the extremes of age may also have related to fears over side effects. Older age groups have greater co-morbidities and therefore are more likely to have perceived that the medication was contra-indicated. Linn et al. also found the elderly were concerned that the medications would worsen existing dizziness.[33] Meanwhile in children, lower participation has been attributed to parents withholding medication due to concerns over potential adverse effects.[11]
Education initiatives regarding LF, the MDA program and common misconceptions have been effective in improving MDA compliance.[34–36] These studies reported that greater LF knowledge reduced the likelihood of declining medication and non-participation, suggesting that these interventions would likely also be effective in Myanmar. The NPELF should consider efforts to improve community education and dispel myths in order to improve MDA participation.
Amarapura had significantly lower levels of MDA participation compared to the other townships in the study. Douglass et al. similarly found low participation in young people surveyed there in 2013 and 2014.[10] This lower participation could not be accounted for by the programmatic reach and compliance factors assessed. Of the four townships, Amarapura is the most urban and had the highest average household income. Studies elsewhere have found that MDA participation can be more difficult to achieve in urban areas because of a lack of urban strategy, fewer peripheral health workers, poor health care infrastructure, the presence of unorganised settlements and large numbers of migrants.[11] Compared to other townships, Amarapura had the highest proportion of individuals who had moved from another village but a similar ratio of household members present during the last round and the highest number of NPELF visits. Within urban areas, studies have also found that higher income individuals can be harder to reach in surveys and are more likely to decline to participate in MDA programs.[11] Amarapura had the lowest proportion of individuals who reported declining MDA medication. When income was assessed in a subgroup analysis of the township, however, there was a trend toward lower participation with higher income but it did not reach significance (cOR 1.07 p = 0.642, aOR 1.41 p = 0.080). The lower participation levels in Amarapura, therefore, may relate to its urban location, more mobile population and higher incomes, but this requires further analysis.
In addition to exploring causes for persistent infection and MDA non-participation, this study also assessed risk factors for LF-related hydrocoele. The positive association found between age and hydrocoele has been well documented.[15] This is thought to be due to the progressive onset of lymphatic dysfunction with chronic filarial infection.[37] Hydrocoele was also found to be associated with CFA positivity but this relationship lost significance following adjustment for survey design. Since individuals with hydrocoele are often CFA negative, this association could potentially reflect an increased risk of hydrocoele development in those with chronic or recurrent infection. The higher risk of hydrocoele in Amarapura probably relates to the historically high infection prevalence there, which is not reflected in current CFA status. These findings underscore the importance of reducing infection to prevent the development of LF-related hydrocoele.
The study results reported should be interpreted in light of some limitations. Firstly, more females than males participated in the study. Whilst gender was adjusted for, it led to wider odds-ratio confidence intervals. Secondly, data was missing from a number of risk factor variables (see total column in Tables 1, 3 and 5) leading to fewer numbers of participants in the final models for infection and never-taking MDA. In addition to widening confidence intervals, it is possible this may have biased the results. Thirdly, other potential environmental factors such as rainfall, temperature and population density were not included, which may have provided a more complete explanation of risk. Lastly, local health workers and members of the NPELF assisted with data collection. It is therefore possible that participants’ responses regarding MDA participation could have been biased towards ‘acceptable’ replies. The low levels of reported MDA participation, however, suggest this was unlikely.
The results of this study will assist Myanmar’s NPELF and contribute to the global understanding of LF risk factors. Knowledge of the factors associated with persistent infection will help the National Program to better allocate its resources in elimination efforts. This should include interventions to improve MDA participation and potentially the screening of household windows and doors. In order to improve participation, our results suggest that emphasis needs to be placed both on improving reach, with particular attention to mopping-up missed participants, and compliance through educational initiatives. Since the findings reflect many common global reasons for poor MDA uptake and those of Linn et al, it is reasonable to infer that they could be generalisable to other regions of Myanmar. The identified infection risk factors may also apply to other countries where Culex is the vector. Finally, the identification of hydrocoele risk factors contributes to the understanding of LF morbidity and will help Myanmar to better target alleviation programs.
{kind=link}