Outbreak overview
From September 2014 to February 2017, a total of 140 vancomycin-resistant Enterococcus faecium (VREfm) cases were identified. Figure 1 shows the epidemic curve of detection of new VREfm-positive patients per week.
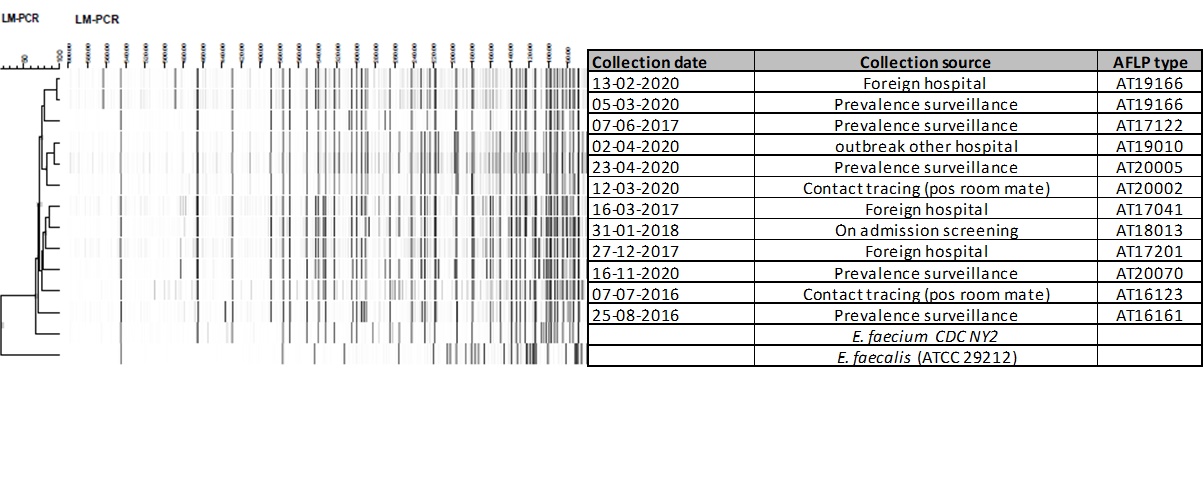
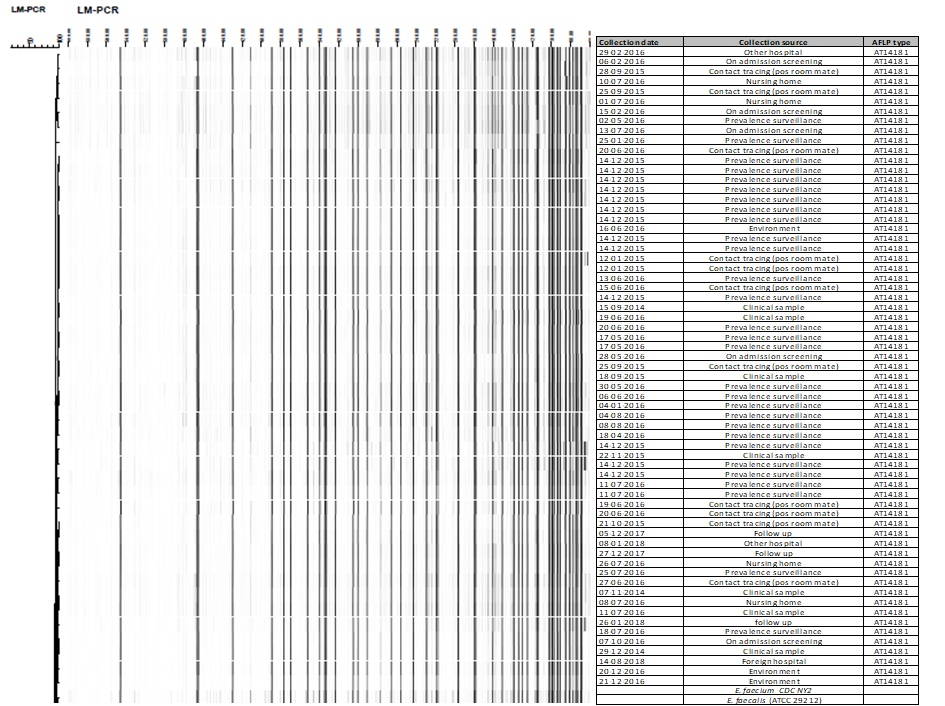
The VREfm strain found during this outbreak expressed a high level of resistance to vancomycin (MIC > 256 mg/L) and teicoplanin (MIC > 32 mg/L) and carried the vanA gene. VRE typing of one of the first isolates showed MLST ST117, designated AFLP type AT14181; subsequent AFLP analysis of 64 isolates in the course of the outbreak period revealed a single AFLP clone (supplementary material S4).
The outbreak was detected in December 2015, where VREfm carriage was found in four patients who had been transferred from location Goes. On December 14, 2015, following the alert from a neighbouring academic hospital, all patients admitted for more than 48 hours were screened for VRE carriage: of the 158 patients screened, 13 patients (8%) were carriers of VREfm. The VREfm positive patients were all admitted to various departments at location Goes (none at location Vlissingen), including the Intensive Care Unit, indicating that VREfm had spread throughout the entire location (with the exception of the AAU, and the children's and maternity ward).
Retrospectively, the start of the outbreak was set at September 1, 2014, as on this date the first VREfm was detected in a clinical specimen of a patient admitted to the surgical ward at location Goes. In the months following September 2014, VREfm strains had been isolated in clinical materials from five patients during their admission to location Goes (Figure 1). These had been at the time considered to be incidental findings without a clear epidemiological link. AFLP typing in December 2015 showed that these isolated belonged to a single AFLP clone (supplementary file S4).
In the first phase out the outbreak from January 2016, VRE suspected patients were isolated with contact precautions (preferably in single rooms) upon (re)admission. Isolation measures were discontinued and the ‘VRE suspected’ label was removed based on a single negative rectal culture. Due to the large number of VRE suspected patients and insufficient availability of single rooms, separate cohorts were formed for VRE positive and VRE suspected patients, each with dedicated rooms, staff and (medical) equipment. Two extra five-bed-rooms were opened on the AAU to accommodate these cohorts by mid-January 2016. On the other wards, VRE suspected or positive patients were placed in a single room or cohorted with other (suspected) VRE carriers if there was insufficient availability of single rooms.
Screening of VRE suspected patients upon admission between January and March 2016 (phase I), showed that only 2 of 647 patients (0.31%) were positive for VREfm. None of these patients were residing in a nursing home or rehabilitation facility. Given the low VRE prevalence in the cohort of patients admitted between September 2014 and December 2015 and the absence of VRE carriage among patients transferred from other institutions, patients from this cohort were labelled ‘medium risk’ and no longer pre-emptively isolated upon admission starting from March 21, 2016 (phase II). Screening of this cohort by performing a single rectal culture upon admission remained unchanged.
In this second phase of the outbreak, patients who had been in contact with a VREfm-positive patient (roommates of VRE carriers) were labelled ‘high risk’, isolated and screened using 3 separate rectum cultures on day 3,5 and 7 after last exposure (table 1).
After an initial decline in the number of new VREfm findings in February and March, 2016 – there was a second peak in the number of VREfm positive patients in May – June, 2016. On-site audits performed during phase II showed shortcomings in infection control preconditions on several wards in the hospital: wards were cluttered, the separation of dirty and clean areas was not clear, and the replacement of damaged hospital equipment and furniture had not been implemented. The division of labour with regards to cleaning responsibilities between cleaning personnel and healthcare workers was further emphasized in this phase, and environmental sampling increased in frequency (see below).
As of November 2016, there were no new VREfm findings in the preceding three months and therefore screening for VRE carriage on admission was limited to only patients with prior hospitalisation in het ADRZ hospital in the period December, 2015 – November, 2016 (phase III). Furthermore, the frequency of hospital-wide screening of patients with >48 hours length of stay was from then on performed monthly instead of weekly.
Control of the outbreak
No further cases occurred over a three months period and control measures were terminated in February, 2017. Admission and prevalence surveillance cultures were discontinued and all outbreak related ‘VRE suspected’ labels in the electronic patient system were removed. Furthermore, a hospital-wide VRE rectal screening limited to patients admitted for at least 7 days, was implemented as a standard surveillance form that moment on.
Environmental cultures
In January 2016, environmental cultures were obtained throughout the hospital to assess the extent of environmental contamination. The cultures showed extensive VRE contamination on the surgical, internal, pulmonary and neurology wards (43/80 samples VRE positive; 53.7%). Environmental samples of the AUU, ICU and dialysis department were VRE negative (0/60 samples). (Figure 2a)
In June 2016, environmental screening was repeated on multiple wards (n = 130 samples), and again extensive VRE contamination was found in the surgical ward (19/20 samples, 95,0%) and to a lesser extent on the cardiology ward (4/20 samples; 20.0%). Consequently, stepwise cleaning and disinfection (250 ppm chlorine) of these wards was performed. After cleaning these wards were closed pending VRE negative environmental results. Following a peak in VRE transmission, environmental surveillance was continued and intensified: from June 2016, rooms previously occupied by VRE-positive patients were only released after cleaning and negative environmental cultures. Ten percent (74/713 culture) of the room surfaces remained VREfm positive after terminal disinfection. (Figure 2b) In some cases, VREfm was still detected after two rounds of terminal disinfection on e.g. patient bed, infusion pole and pull-up bar.
Infections during the outbreak period
Eight (5.7%) patients developed a VREfm infection, of whom two (1,4%) had bacteraemia. Two patients, with extensive co-morbidities, died shortly after detection. One patient, also with extensive co-morbidities (including renal failure, haemodialysis and vascular disease) developed a severe osteomyelitis following a surgical procedure, which eventually led to amputation of her left hand.
{kind=link}
{kind=link}