Study design and population
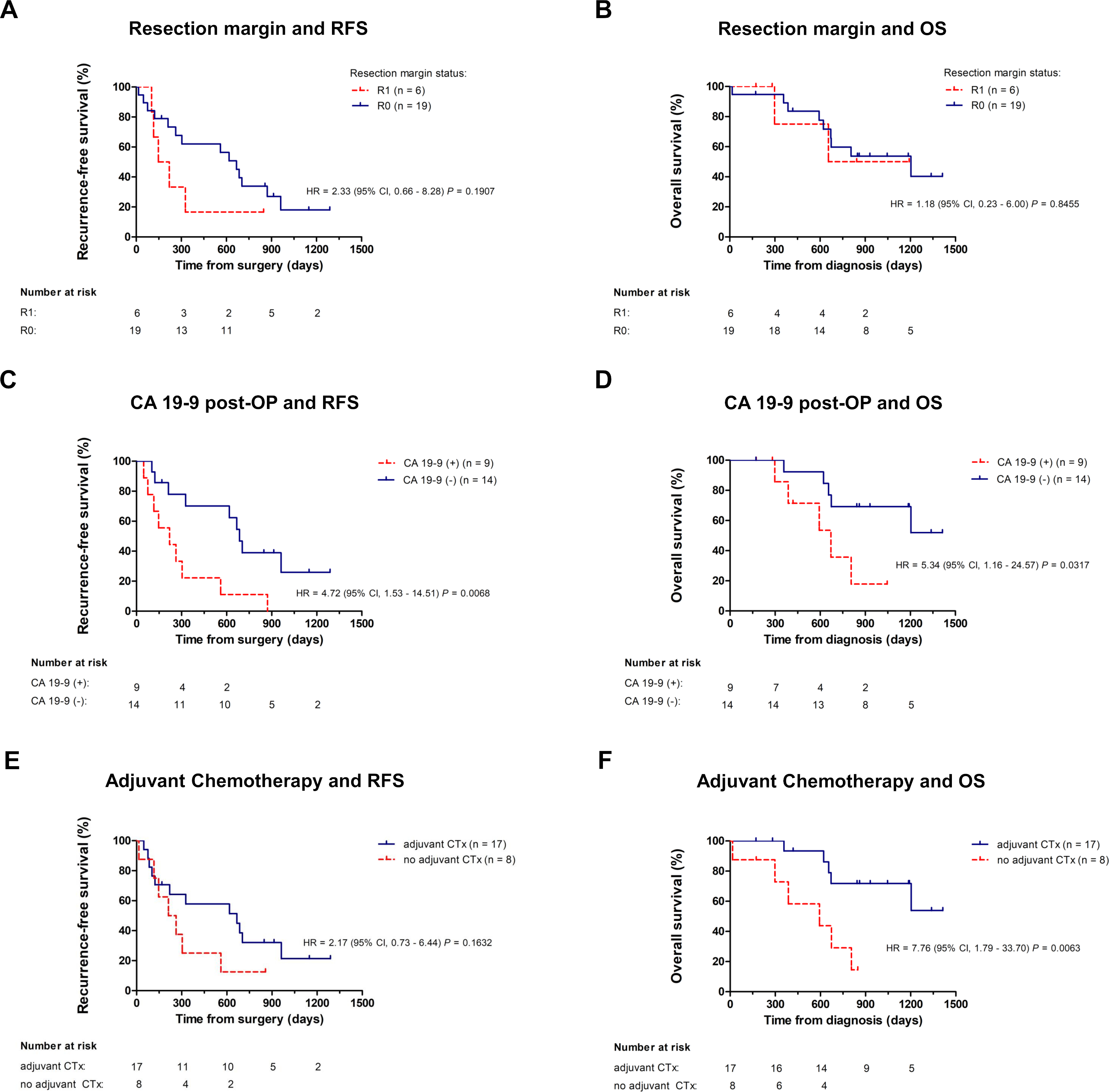
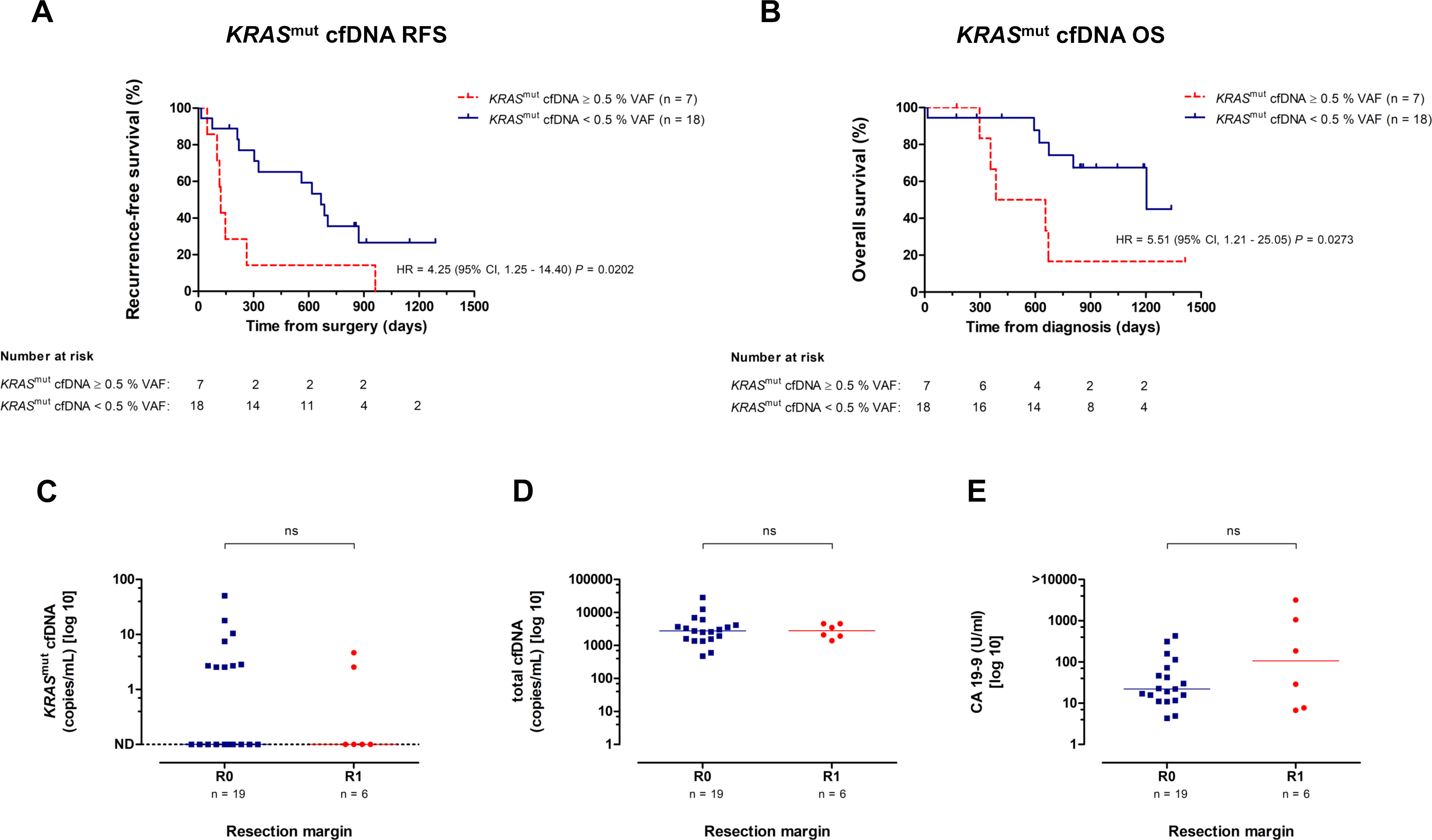
25 patients with resected pancreatic adenocarcinoma (following R0 or R1 curative-intended resection) were included in a retrospective observational single center biomarker study conducted at Freiburg University Medical Center. Local institutional review board (IRB) approved all study procedures (EK48/18). All patients provided written informed consent for sample collection and analysis. 17/25 patients underwent adjuvant chemotherapy (4/17 Gemcitabine, 4/17 FOLFIRINOX, 8/17 Gemcitabine/Capecitabine, 1/17 Gemcitabine/nab-Paclitaxel). Further inclusion criteria were “collection of first sample within 8 weeks after resection”, and “availability of plasma samples for cfDNA extraction”. Key exclusion criteria included “R2 resection, evidence of metastatic disease on pre- or postoperative CT staging, histologies other than adenocarcinoma”. According to UICC/AJCC, R0 resection was defined as microscopic edge-negative resection, in which no microscopic residual tumor remains. R1 resection was defined as a microscopic residual tumor and R2 as macroscopically visible residual tumor. Primary endpoint was detection of cfKRASmut in at least one sample during study period. Secondary endpoints included association between changes in cfKRASmut and relapse-free survival (RFS) and overall survival (OS). Additionally, clinical, pathologic, treatment- and outcome-related data were analyzed.
Collection of patient samples and CA 19-9 analysis
Blood samples were collected at a median of 40 days (95% CI 26-50) after resection, prior to adjuvant chemotherapy and during 3-monthly routine clinical follow-up visits. CA 19-9 measurements were performed at our center`s fully certified clinical chemistry facilities. The threshold value for CA 19-9 positivity was 36 U/ml.
Extraction of cell-free DNA (cfDNA) from plasma samples
Blood samples were collected using commercially available EDTA tubes and plasma was extracted and frozen within one hour of collection. Plasma was extracted through two subsequent centrifugation steps at 3000 rpm and 14000 rpm, each for 10 min at 4°C. Obtained plasma was stored at -80°C until extraction of cfDNA. cfDNA was extracted from 4ml plasma following the SEP/SBS protocol of the PME-free circulating DNA extraction kit (Analytik Jena, cat. no. 845-IR-0003050), following manufacturer’s instructions. Two subsequent elution steps with each 30 µl Elution Buffer were performed to optimize the yield of extracted cfDNA. DNA was stored at -20°C until cfDNA quantification. cfDNA was evaluated with fragment analyzer and quantified using Qubit 2.0 fluorometer. In patients with resectable PDAC, DNA yield from 4ml of plasma typically ranged from 1 to 20 ng/µl.
Droplet digital PCR (ddPCR)
ddPCR for cfKRASmut was performed as recently described [29]. Locked nucleic acid (LNA) probes and corresponding primer pairs for KRAS mutations were designed using Beacon Designer v.8.20 software (Premier Biosoft, Palo Alto, California, USA) and manufactured by Integrated DNA Technologies (IDT, Inc., Coralville, Iowa, USA). Wild type (WT) probes were labelled with hexachlorofluorescein (HEX), mutant (MUT) probes with 6-carboxyfluorescein (FAM). Primer and Probe sequences are listed in Supplemental Table 1. Primers, probes, template DNA and nuclease-free water (Ambion, Austin, TX) were added to ddPCR Supermix for Probes (Bio-Rad, cat. no #186-3024). Reaction mix was set up as recommended. 20 µl of this reaction mix along with 70 µl reader oil were transferred into cartridges of a QX100/200TM Droplet Generator (Bio-Rad, cat. no. #1863002) following manufacturer’s instructions. All samples were assayed in quadruplicates. Droplets were generated, transferred into a 96-well PCR plate (Bio-Rad, cat. no. #12001925) and PCR was then run on a C1000 TouchTM Thermal Cycler (Bio-Rad, cat. no. #1851197). Finally, samples were analyzed on a QX100/200TM Droplet Reader (Bio-Rad, cat. no. 1863003) using QuantaSoft v1.7.4.0917 (Bio-Rad, cat.no. #1864011). Internal ddPCR controls were carried out as previously published [29].
The absolute number of copies per milliliter of blood were calculated as follows: Copies/mL plasma = (copies per µL of reaction as per QuantaSoft analysis software version 1.7.4.0917) × (volume of ddPCR reaction) × ([volume eluted/volume of DNA used in reaction]/volume of plasma used for cfDNA extraction). Mutant allele frequency was calculated as: Mutant allele frequency = mutant copies/mL of plasma / (mutant copies/mL of plasma + wild−type copies/mL of plasma).
Limit of detection (LOD) and limit of blank (LOB) of the individual assays have been previously described [30] .
In brief, cfDNA was screened for the presence of the 11 most commonly found KRAS hot spot mutations, in PDAC, covering more than 90% of PDAC cases. Highly sensitive single-target assays were used to confirm presence of the mutation identified.
Statistical analysis
Recurrence-free survival (RFS) was defined as time from resection of PDAC to the first radiologic recurrence (local or distant) or death due to PDAC. Overall survival (OS) was defined as time from the date of diagnosis until death due to any cause. The Kaplan–Meier survival analysis was performed to calculate both RFS and OS. Univariate analyses were performed using the log-rank test. In order to explore independent prognostic factors for RFS and OS, we used backward stepwise Cox regression modeling to estimate hazard ratio (HR) with 95% confidence interval (CI). To compare independent variables, Chi-squared or Fisher’s exact test and the Mann–Whitney (rank-sum) test were performed. All statistical analyses were performed using GraphPad Prism Version 5.03 (GraphPad Software, Inc., La Jolla, California, USA) and SPSS 25 software Version 1.0.0.1327 (IBM Corporation, New York, United States). P values < 0.05 were considered as statistically significant.
{kind=link}
{kind=link}