- IN VITRO STUDY
a. Cell lines and culture conditions
The human ovarian cancer cell lines PA-1, Caov-3 and SK-OV-3 were obtained from ATCC (LGC Standards S.a.r.l., France). SK-OV-3LucIP1 cells were selected in vivo (11) and together with the NIH:OVCAR-3 cell line provided by the LECR research group (Ghent University, Belgium). This cell panel was extended with the patient-derived xenograft-derived low-grade serous ovarian cancer cell line PM-LGSOC-01(12). SK-OV-3 cells were maintained in ATCC-formulated McCoys 5A medium, SK-OV-3LucIP1 and Caov-3 cells in ATCC-formulated Dulbecco's Modified Eagle's Medium (DMEM) and PA-1 together with PM-LGSOC-01 cells in ATCC-formulated Eagle’s Minimum Essential medium (EMEM). NIH:OVCAR-3 cells were maintained in RPMI-1640 Medium (Life Technologies, Belgium). All growth media were completed by adding 10% fetal bovine serum (FBS) and antibiotics (penicillin/streptomycin), and incubated at 37 °C with 5% CO2 in air.
SK-OV-3 represents the parental cell line of SK-OV-3lucIP1, the SK-OV-3 cell line was established based on ascitic fluid from a 64-year-old woman. SK-OV-3 cells were derived from an adenocarcinoma and carries mutations in TP53 and PIK3CA. The SK-OV-3lucIP1 cells were established after one intraperitoneal passage of SK-OV-3luc cells in mice, as described by De Vlieghere et al. (11). The PA-1 cell line presents with an NRAS mutation and is derived from a 12-year-old girl diagnosed with a teratocarcinoma or ovarian mixed-germ cell tumor. Both Caov-3 and NIH:OVCAR-3 were derived from an ovarian adenocarcinoma. Caov-3 cells were established from a 54-year-old woman and carry mutations in TP53 and PIK3CA whereas NIH:OVCAR-3 cells were derived from a 60-year-old woman and present with a TP53 mutation. The PM-LGSOC-01 cells were derived from a peritoneal metastasis-patient derived xenograft model established based on fresh tumor tissue from a 60-year-old woman suffering from low grade serous ovarian cancer, as described by De Thaye et al. (12). These cells do present a KRAS mutation.
b. Drug treatments
Cells were suspended in culture medium and added to a 96-well plate in a volume of 200 µL with a concentration of 6 000 cells. Cells were allowed to attach for 72 hours before treating them with paclitaxel (PTX, Enzo Life Sciences BVBA, Belgium). A 1% EtOH-solution in complete growth medium was used as control solution (0 nM) and vehicle for PTX-containing solutions. PTX concentrations in the clinically relevant concentration range of 1 to 1 000 nM(13) were studied. After incubating the cells with 0, 1, 10, 100 or 1000 nM PTX for 24 hours, wells were washed with phosphate buffered saline and complete growth medium before adding 200 µL of fresh complete growth medium. Every 24h, up to 120h after PTX treatment, medium was collected, levels of released ccCK18 biomarker were measured and an MTS assay was performed. For every concentration and time point, the experiment was performed in fourfold.
c. MTS assay
The MTS assay was performed according to the manufacturer’s instructions, using the CellTiter 96® AQueous One Solution cell proliferation assay (Promega, USA). Absorbance was measured at 490 nm using the Infinite® M200 PRO NanoQuant plate reader (TECAN, Switzerland). Cell counts were assessed by performing MTS assays in the presence of standard curves using increasing cell amounts.
d. Assessment of ccCK18 by ELISA
The cell culture medium aspirated from the wells was first centrifuged for 5 min at 1000 rpm and then aliquoted and stored at –80 °C until analysis. In order to be certain that only cell-free supernatant was collected, an examination under the AE2000 binocular microscope (Motic Instruments Inc., Canada) was performed. Levels of ccCK18 were quantitatively determined, according to the manufacturer’s instructions, using the M30 Apoptosense® ELISA kit (PEVIVA, Sweden).
e. Cell lysates and Western blot analysis
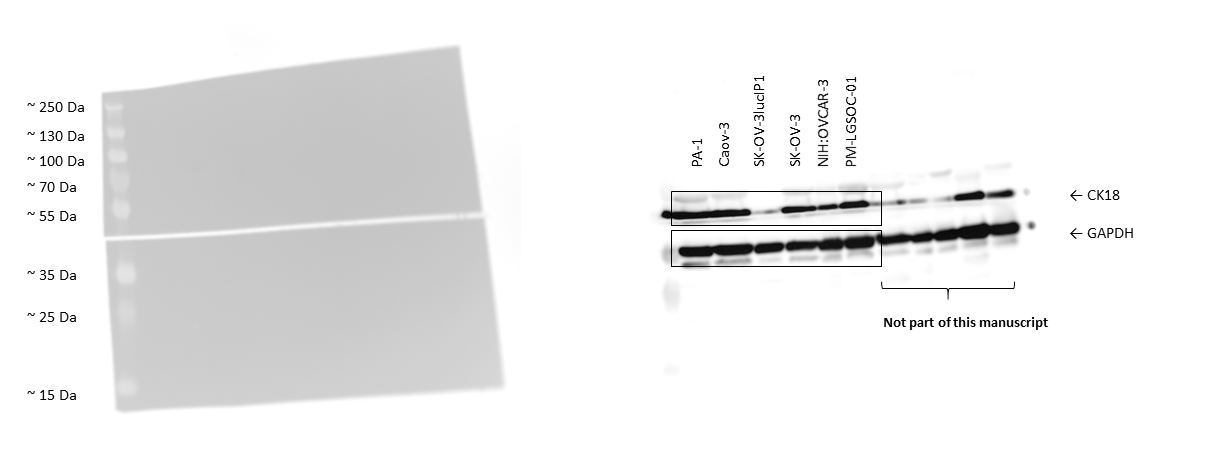
Proteins were extracted from untreated cancer cells using the Laemmli lysis buffer (0.125 M Tris-HCl, 10% glycerol, 2.3% sodium dodecyl sulfate (SDS), pH 6.8). Cell lysates were suspended in reducing sample buffer (1 M Tris-HCl, 30% glycerol, 6% SDS, 3% β-mercaptoethanol, 0.005% bromophenol blue, pH 6.8) and boiled for 5 minutes at 95°C. 25 µg proteins of each cell line were exposed to a 10% SDS-PAGE gel and transferred to nitrocellulose membranes (Bio-Rad, Hercules, CA, USA). After blocking the membranes using 5% non-fat milk in phosphate-buffered saline (PBS) with 0.5% Tween® 20 (Sigma-Aldrich, Belgium), the blot was incubated overnight at 4°C with mouse monoclonal anti-human cytokeratin 18 (R&D Systems, United Kingdom). After washing the membrane, incubation with HRP-conjugated anti-mouse IgG secondary antibody was performed at room temperature for 1 hour. The WesternBright Quantum HRP substrate (Advansta, Menlo Park, CA, USA) was added to the membranes to capture the luminescent signal using the Proxima 2850 Imager (IsoGen Life Sciences, De Meern, The Netherlands). Equal loading of samples was verified by primary antibodies mouse monoclonal anti-GAPDH (clone GAPDH-71.1, Sigma-Aldrich, Belgium).
f. Phase-nonspecific pharmacodynamic model for cell count
Cell count data were analyzed using a phase-nonspecific pharmacodynamic model with NONMEM® (version 7.3.0, ICON, Hanover, MD, USA) based on the work by Mouton et al. (1997)(14), Nielsen et al. (2007)(15) and Rao et al. (2016) (16).
See formula 1 in the supplementary files.
where N refers to the cell number, t is time, kng is the net growth rate constant and Emax refers to the maximum PTX-induced treatment effect. Conc refers to the concentration of PTX to which cells were exposed and C50 denotes the concentration at which half of the maximum effect is reached.
There was also a term base_count included in this model to take into account the estimated cell numbers present before treatment with PTX. Population parameters and error variance were estimated using the first-order (FO) estimation routine.
g. Phase-nonspecific pharmacodynamic model for released ccCK18 levels
The ccCK18 release data were also analyzed using a phase-nonspecific pharmacodynamic model with NONMEM® (version 7.3.0, ICON, Hanover, MD, USA). The term kprod was used here as the net production rate constant of extracellular ccCK18. Parameters such as the maximum amount of released marker (Amax) and the Hill coefficient γ, to describe the steepness of the relationship between PTX concentration and response, were added. A refers here to the extracellular amount of ccCK18.
See formula 2 in the supplementary files.
Also here the base_amount term was included in the model to estimate the initial amount of released ccCK18 before exposure to PTX. Population parameters and error variance were estimated using the first-order (FO) method.
2. IN VIVO STUDY
a. PA-1 and SK-OV-3LucIP1 xenograft models
The human ovarian cancer cell lines PA-1 and SK-OV-3LucIP1 cells were used to xenograft SCID/Beige mice (mice were commercially obtained from Envigo, The Netherlands). SK-OV-3LucIP1 cells were cultured in ATCC-formulated Dulbecco's Modified Eagle's Medium (DMEM) and PA-1 cells in ATCC-formulated Eagle’s Minimum Essential medium (EMEM). All growth media were completed by adding 10% fetal bovine serum (FBS) and antibiotics (penicillin/streptomycin). Cells were incubated at 37 °C with 5% CO2 in air. 7 to 9-week-old female SCID/Beige mice were unilaterally subperitoneally injected with 1×106 cancer cells (1:1 serum free medium:Matrigel (Corning, The Netherlands). In total, 20 PA-1-xenografted mice and 30 SK-OV-3LucIP1-xenografted mice where studied. The control groups were based on 10 PA-1- and 15 SK-OV-3LucIP1-xenografted mice, respectively. The maximum caging density was 6 from the same experimental group. All mice were maintained on a regular diurnal lighting cycle (12:12 light:dark) with ad libitum access to food and water. Mice were monitored once every day.
b. Single dose study
Mice were randomly assigned to the placebo or treatment group after subperitoneal tumor cell injection. PTX (Abraxane®, Celgene, US) was intraperitoneally (ip, 50 mg/kg) administered to the treatment group 2.5 weeks after tumor cell injection whereas the control group received an intraperitoneal injection of 0.9% NaCl (placebo) in an equal volume at the same time. Whole blood was collected via cardial puncture in K3EDTA-treated Sarstedt (B.V.B.A. Berchem, Belgium) Microvette® 200 tubes, prior to obtain plasma. Samples were collected up to 2 weeks after PTX administration to measure ccCK18 levels. Blood collection via cardial puncture was considered a terminal procedure before mice were euthanized using an isoflurane overdose prior to cervical dislocation. Every individual mouse was considered an experimental unit in this study. The animals were excluded from the study if no tumor was present 2.5 weeks after tumor cell injection, which was not the case here.
c. Measurement of tumor volume
Tumor volume in xenografted mice was assessed using ultrasound imaging. Transparent ultrasound transmission Polaris II gel (Ondes & Rayons Medical, France) was applied to bare skin and a MicroScan™ MS550D (22–55 MHz, VisualSonics Inc., Canada) transducer with the Vevo® 2100 imaging system (VisualSonics Inc., Canada) was used to analyze the tumor volume in Vevo LAB 1.7.1 (VisualSonics Inc., Canada). Tumor volumes (in mm³) were measured before receiving the single dose of PTX and before the cardial puncture at the time of sacrifice.
d. Tissue processing and immunohistochemistry
Tumor tissues collected from mice were fixed overnight in neutral buffered 10% formalin solution (Sigma-Aldrich, Belgium) and processed in the tissue core facility at Ghent University Hospital.
e. Assessment of caspase-cleaved CK18 by ELISA
Collected plasma samples were aliquoted and stored at –80 °C until analysis. Levels of ccCK18 were quantitatively determined, according to the manufacturer’s instructions, using the M30 Apoptosense® ELISA kit (PEVIVA, Sweden).
{kind=link}