Primarily due to cardiovascular comorbidities patients with RA die significantly earlier [7, 15] the risk of sudden cardiac death is doubled in RA compared to the general population [16, 41–43]. Due to the accelerated cardiovascular risk, the precise risk evaluation is essential. Our present data confirm and extend previous observations regarding the increased cardiovascular risk in RA. Here we show for the first time the profound effect of RA on the arterial age, compared to the MESA population. Older arterial age was associated with smoking, previous cardiovascular events and hypertension. The follow-up substudy was self-controlled and highlighted the importance of other additional factors. Ongoing inflammation (CRP > 5 mg/L) especially in smokers and shorter disease duration (< 10 years) accelerated arterial aging according to our follow-up data. Therefore, the increased cardiovascular risk due to RA increases with the disease years but the augmentation is not linear, in the first 10 years of the disease the arterial aging is apparently more pronounced.
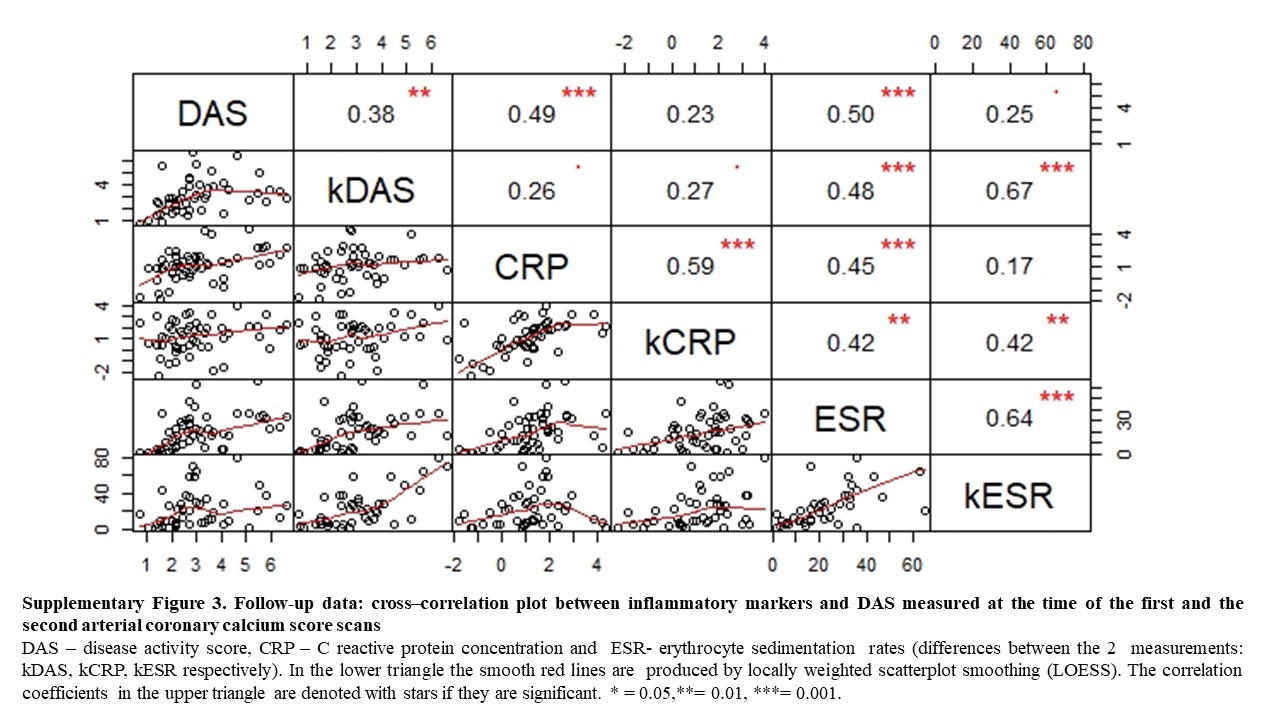
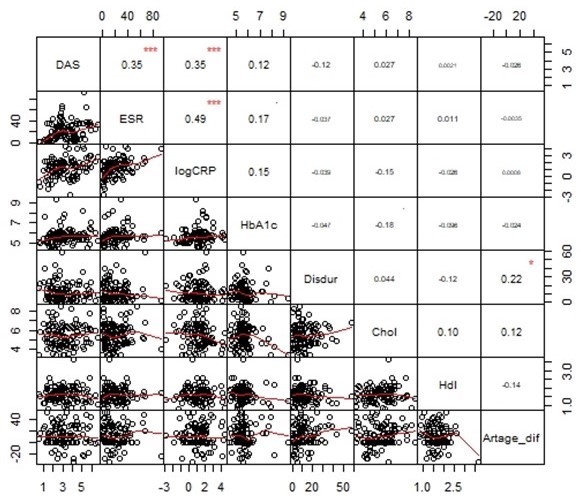
Inflammation plays a central role in the pathogenesis of atherosclerosis; elevated levels of C-reactive protein (CRP), interleukin-6, and N-terminal pro-hormone B-type natriuretic peptide (NTproBNP) correlate closely with cardiac events [44]. Epidemiological studies suggested that chronic inflammation is associated with higher cardiovascular risk. In addition, inflammation is a recognized risk factor of AMI in RA [45]. A number of inflammatory mediators have been widely studied, both as surrogate biomarkers and as causal agents, in the pathophysiological network of atherogenesis and plaque vulnerability [46]. Low disease activity is associated with a decreased risk of CVE in RA [47] In patients with RA, inflammatory markers, disease severity, and RF positivity, were found to be associated with the risk of atherosclerosis [48]. ACPA and RF are both unfavorable prognostic factors in RA, in accordance with our present data both autoantibodies are independent from the accelerated arterial aging in RA [49].
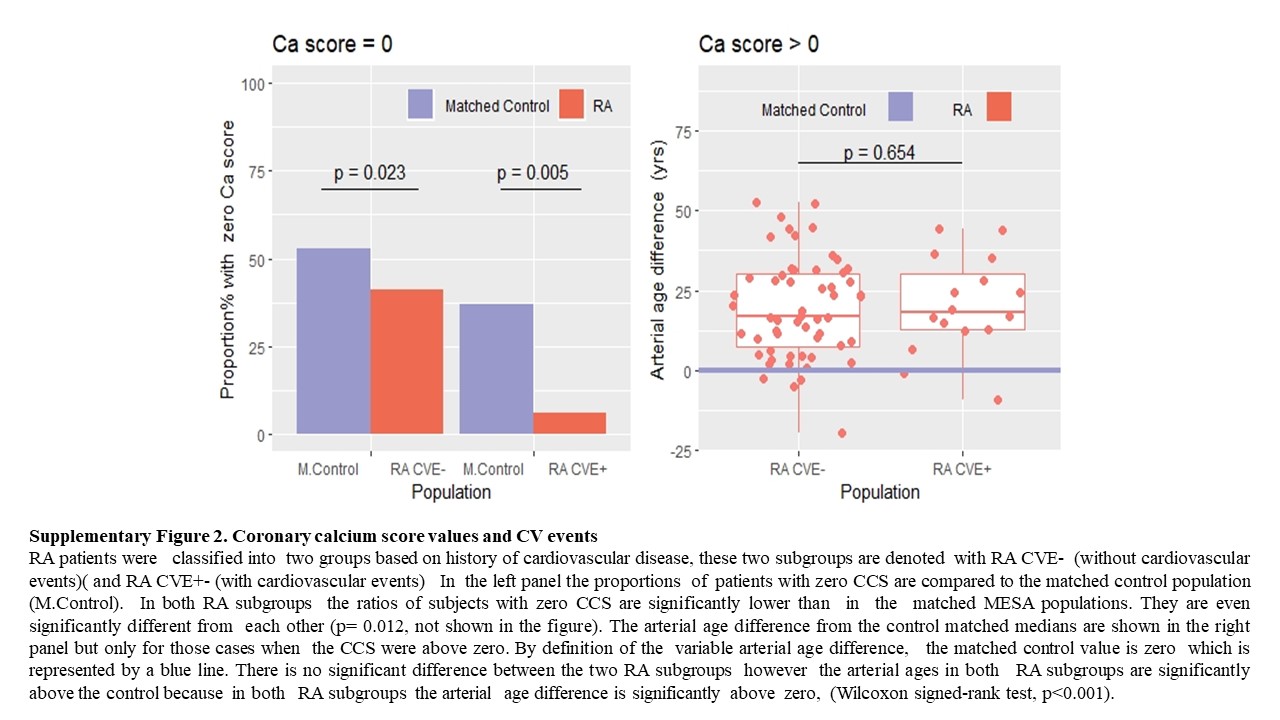
The age is an independent risk factor for cardiovascular diseases, nevertheless often the atherosclerotic disease burden is discordant with a patient’s chronological age. Calcium is a general component of the atherosclerotic plaque, but not that of the normal vessel wall [23]. Because of this structural difference, the calcium is an accurate index of atherosclerotic disease burden and a useful tool to estimate the risk of cardiovascular adverse outcomes [27, 50]. Previous studies showed the importance of age specific CCS percentiles to predict the occurrence of a cardiovascular event in patients with a similar risk profile [51]. CCS is a widely accepted marker of coronary atherosclerosis. In the MESA population, a doubling of the CCS increased the probability of a coronary event by 25% in a 3.8-year follow-up period. Importantly, this predictive value was relatively stable across different ethnic groups [52]. Similarly to our present data, RA severity was associated with the greater prevalence of coronary artery calcification compared to the MESA population [20]. The Framingham risk score includes age, gender, total and HDL cholesterol, blood pressure, diabetes, and smoking. However long-standing RA had higher Framingham risk scores compared with patients with early disease or control subjects. Furthermore, longstanding inflammation represent additional cardiovascular risk [53]. Moreover, the presence of CAC has been shown in early RA as well [54]. The lack of diabetes effect in our study was somewhat surprising because it is generally presumed that the CCS is independently associated with incident coronary heart disease in diabetes [55]. Framingham risk based on arterial age is more predictive of short-term incident coronary events than Framingham risk based on the observed age [37].
According to recently published data, coronary artery calcification increases with higher total prednisone dose, by contrast methotrexate and other csDMARDs do not influence coronary plaque progression [33]. Furthermore, DMARD and TNF-α antagonists are associated with reduced risk of myocardial infarction, stroke and cardiovascular death [56, 57]. In the present study we did not find any significant effect of the anti-inflammatory or lipid lowering therapies. However, the limited study power prohibits to draw any definite conclusions regarding the effect of statins and targeted therapies on arterial aging. There are other limitations of our work as well: most of our patients had moderate disease activity and untreated patients with early disease were not included in this study.
{kind=link}
{kind=link}
{kind=link}